Healthy versus Toxic Contracts

Conversations and Independent Contract
Audits Can Create Ethical and Effective
Fee-For-Service, Alternative-Payment Methods & Value-Based Payment Contracts
This article requires study. There are many purposes for this paper, the most important is to encourage mental and behavioral health professionals to ask questions and learn more about fee-for-services (FFS), alternative payment methods (APM), and value-based payment (VBP) contracts; to support understanding of the ways pay-for-performance (P4P), measurement-based care (MBC), and outcome informed care (OIC) are necessary foundations for mental and behavioral healthcare contract design and implementation.
Mentor Research Institute, 501c3
(Draft v1.8, January 1, 2024)
Oregon licensed mental and behavioral health professionals are encouraged to READ & SIGN the Healthy Contracts Petition
Summary
The Oregon Legislature through Senate Bill 889 (2019 Law) and House Bill 2081 (2021 Law) has established the Sustainable Health Care Cost Growth Target Program within the Oregon Health Authority (OHA). The cost of health care in Oregon has grown and is projected to grow faster than both the state economy and Oregonians’ wages. The voluntary allowable increase target set by the OHA and adopted by the Oregon Value-Based Payment Compact is 3.49%.
One Healthplan (hereafter referred to as Healthplan X) subsequently proposed a contract with a behavioral health incentive program (BHIP). Healthplan X had taken an approach to increase the quality and effectiveness of mental health services by promoting measurement that offers financial incentives to professionals so that Healthplan X presumably can evaluate providers’ practices, i.e., access, efforts to coordinate care, effectiveness, and quality improvement. The expectations and requirements are ill-defined and vague at best. Healthplan X proposed that quality factors will increase efficiency in turn will increase the ability of providers to see more patients. However, there is no evidence that the “value” of outcome measurement will increase access. The contract is at best an uncontrolled and ill-designed experiment. Mentor Research Institute (MRI) proposed to Healthplan X that the mental and behavioral health workforce needs to be expanded, new providers recruited and offered contracts structured for their participation during their pre-licensure period, and that the services of current mental and behavioral health professionals should be retained by Healthplans rather than risk being lost by intimidating and alienating contracts language and requirements which lead qualified professionals to either “game” contracts” or the choice of working primarily or only “out of pocket.” MRI proposed, based on 20 years of experience training mental health professionals, that labor force issues are separate from models of care that include measurement and payment models such as APM and VBP.
Healthplan X contract and requirements were the subject of an independent audit initiated by MRI. The result concludes that Healthplan X’s contract has a probable to almost certain risk of failing to improve access to care or improved quality of care and outcomes. This conclusion is attributed, in part, by Healthplan X refusal to (1) have conversations, (2) establish shared definitions of values, (3) create shared objectives that can achieve those values, (4) allow providers to create baselines for population specific treatment models, (4) create transparent “controls”, (5) create transparent “test scripts”, and (6) refusal to co-create “key performance indicators” (KPI).
American Mental Health Alliance Oregon (AMHA-OR) renamed itself in October 2023 as Independent Mental Health Practices Alliance (IMHPA). IMPHA is capable of moving toward and into VBR, MBC, and OIC. That is a necessary first step before incentives should be offered. IMPHA is a group contract capable organization comprised of independent mental, behavioral and substance abuse treatment providers. IMHPA conducted a focus group of members and guests to expand on beliefs important to mental, behavioral and substance use treatment services, recognizing that:
According to the American Psychological Association, categories of quality, for purposes of mental and behavioral health, are defined by (a) infrastructure, (b) practice processes, and (c) outcomes.
The Oregon Health Authority (OHA) has defined values specifically as (a) “evidence-based”, (b) “patient-centered”, and (c) “improved quality and positive health outcomes at an appropriate cost”.
The Oregon Value-Based Payment Compact (OR-Compact) has defined “values” specifically as (a) “evidence-based”, (b) “patient-centered”, and (c) “increased effectiveness at a reduced cost”.
MRI has provided leadership to provider practices in defining best practices that incorporate measurement utilizing a provider and Healthplan friendly technology platform which adheres to the shared values outlined above. Equally important is development of a payment methodology that compensates providers for their expertise and their commitment of time and effort to quality improvement and value-based objectives. In January 2022, MRI proposed to Healthplan X a model of appropriate increased rates for each of the relevant CPT codes for mental health and substance use services. The proposal reflected cost, and recommended reimbursement rate competitive with other payers. At a minimum, FFS, OIC, MBC, APM and VBP require use of an interactive complexity code (CPT 90785) and a measurement CPT code (CPT 90899).
The OHA defines as “evidenced based”, “patient-centered and “improved quality and positive health outcomes at an appropriate cost.s” The Oregon Value-Based Payment Compact (ORCompact) disagreed and redefined it as “Increased effectiveness at a reduced cost.” The values of “increased effectiveness at a reduced cost” and “improved quality and positive health outcomes at an appropriate cost” are not synonymous. This mismatch is just one example out of 42 reasons Healthplans in Oregon struggle with provider practices to create value-based services. Contracts are structured to benefit Healthplan values (e.g., profit and market share) which benefit Healthplans consistently to the detriment of providers services and the public access. Healthplan X created a contract of adhesion (i.e., take-it-or-leave) which is unfair and is not negotiated in good faith. The Audit concluded that if nothing is changed there is a probable to almost certain moderate to catastrophic impact on the achievement of OHA sustainable Healthcare values and maximum allowable cost growth of 3.49%.
Based on an independent audit of Healthplan X’s contract proposal it has become clear that FFS, APM and VBP contracts require auditing before they should be signed. Provider practices lack the legal, technical, and financial resources to understand, create conversations, and challenge or negotiate contracts with Healthplans. Provider practices lack bargaining power. Healthplans refuse to answer questions and have conversations. Contract auditing involves independent objective assurance, and consulting activity required of both payers and providers, a process designed to define and add value, to meet shared objectives, improve contracted operations, effectively manage contract cycles, and protect ethical provider practices. This focus gives providers information necessary to make information informed decisions. The purposes of contract auditing is to support partnership by supporting transparency, objective data informed decisions that are evidence-based, deliver care that is patient-centered, which supports measurable improvements in quality and health improvement at appropriate cost.
Contracting Requirements for P4P, MBC, OIC, FFS, APM, VBP
Requirements P4P, MBC, OIC, FFS, APM, and VBP for mental and behavioral health practices:
Collaboration drives innovation in practice and financial models.
A Healthplan must challenge itself to clearly define what is of “value” in its mental and behavioral health contracts.
Models of practice and workflows are provider centered.
Measurement is provider and patient-centered.
Collaboration (i.e., conversation) between payers, providers, and patients is important to achieve equity and quality targets.
Reimbursement rates need to be competitive.
Patient access is a function of supply, demand, and provider opportunity cost.
Measurement-based care (MBC) does not address access and is only one aspect of quality-value.
Existing payment methodologies reflect fee-for-service, case rates, episodes of care rates, per member per month, and added incentive payments structured to support MBC, alternative payment methods (APM) and value-based payment (VBP).
Health Plan payment methodologies need to be clearly defined, transparent and auditable.
Contracting for the lowest price is based on payer and provider willingness to agree to those price terms.
MRI and IMPHA recommend that quality services be provided at a rate which reflects the expertise, investment of resources, and competence of providers building a baseline that can be used to set benchmarks as a basis for quality improvement.
Healthy contracting requires “good faith” and “fair dealing.” Toxic contracting is the result of “bad faith” and “unfair risk”. Toxic contracts create toxic outcomes which are unreliable, not accountable, and reduce access to medically necessary care which Healthplans are causing because providers protests and requestions for conversation are ignored.
Effective contracting for FFS, APM and VBP must include a reliable, valid, and useful estimate of risks impacting objectives and key performance measures so that neither Healthplans or provider are unknowingly set up to fail. Healthplan’s performance can be measured in lawful ways that create public confidence with legislative regulation.
When providers are devoted to providing care for patients believe a contract is rigged to deny access and to fail, and they are unable to renegotiate based on data, the contract is unfair and created in bad faith. Such contracts are ineffective, unenforceable, can be voided, and are vulnerable to “gaming”, boycott, and class action lawsuits.
Healthplan contracts which do not (1) share values, (2) shared objectives, (3) have transparent “controls” (management methods), (4) have “test scripts”, and generate (5) key performance indicators" threaten public health, such contracts waste taxpayer and employer dollars, limit access to care, and undermine measurable improvements by mental and behavioral health practices.
Legislative Recommendations
Mental and behavioral health providers’ practices do not have the legal and financial resources to hold Healthplans and other payers accountable for contracts and policies that threaten individual patients and public health. Mental and behavioral health professionals are first to identify Healthplan waste, policies and actions that undermine best practices, and to recognize the services necessary to create positive outcomes. Provider practices are a front line of care and a first line of defense for vulnerable mental and behavioral health clients.
MRI recommends that providers seek legislative requirements for Healthplans to pay the cost of a consulting Certified Internal Auditor (CIA) or equivalent to serve as an independent contract auditor. The Audit Officer (AO) should report to a Mental and Behavioral Health Practices Contract Audit Committee (CAC), not to Healthplans, and especially not to Healthplans’ legal departments. The composition of the CAC should include independent practice providers, group practice providers, clinician representatives of mental health services employers, and 2 representatives of Healthplans.
Mental and behavioral professionals who are candidates for the CAC should be selected based on (1) their type of practice, (2) knowledge of P4P, MBC, APM and VBP contracting, (3) recommendations of peers, (4) knowledge of behavioral health research and design, and (5) experience working on committees or boards.
A CAC consisting of 8 professionals licensed in Oregon as mental health professionals should be empaneled by the legislature. The committee would include 6 independent and employed mental and behavioral health professionals. The CAC would also include 2 licensed mental health professionals acting as representatives of Healthplans.
The CAC working with an AO will be responsible for establishing the scope of audits, setting audit priorities, approving audits, reviewing, and authorizing publication of AO reports to Healthplans, providers, and the public. The CAC will be responsible for developing and setting the annual audit action plan. The CAC will not investigate the internal operations of Healthplan but will interview Healthplans to obtain the information which provider practices need to make informed decisions about contracts. Provider practices should not be asked to sign contracts they do not understand and cannot afford to evaluate, negotiate, or challenge. Annual budgets for electronic publications and reporting to the provider practices and OHA should be established and funded by the OHA by assessing all Healthplans an annual nominal fee.
Examples of actual Healthplan contract requirements that represent potential reasons for a CAC independent audit:
The Healthplan changes their compliance audits procedures for chart notes in ways that are not transparent, preventing provider practices from knowing what they were audited against (i.e., An independent auditor therefore cannot follow the same procedure (i.e., scripts) used by the Healthplan and come to the same result.
The Healthplan contract does not explicitly state their authority to lower rates and the plan lowers rates “at will” without notifying practice providers. Practice providers must, in some cases, give 120 days notice before they can terminate their contracts and be paid the lower rates for that time.
The Healthplan has contract language and requirements that are ill-defined and the consequences are “material” to the provider. Material consequences might include anything that could increase provider work and expenses including arbitrary changes in their incentives in the middle of what could be an indeterminant contract cycle.
The Healthplan requires the provider to use CPT codes for clinical services that are not appropriate and denies use of codes that are appropriate for billing and establishing baselines.
The Healthplan hires a 3rd party operational support service to send intimidating letters to providers threatening to report providers to the Healthplan for what seems to be an arbitrary reason that is intimidating and unnecessary. These letters target providers who use certain billing codes that are deemed to be excessive in use based on statistical analysis rather than a clinical analysis.
The Healthplan offers an incentive for providers and sets a performance target that the providers have no ability to achieve because the target is entirely under the control of the Healthplan, NOT the provider’s practices.
The Healthplan requires provider practices to self-audit and attest that they are compliant with Oregon Administrative Rules that the Healthplan does not understand, and that the State cannot explain or define (i.e., The regulation is not sufficiently defined).
The Healthplan audits provider practices based on criteria that is not transparent, deems the record inadequate, and assesses money that must be returned to the Healthplan before the provider can appeal the decision.
Healthplans should be prohibited from implementing new contracts, or making changes to contracts, until providers have 60 days (post audit) to review and comment on the audit. Contract provisions that do not support OHA values and objectives and/or have no value or may harm public health will not be implemented without successful clarification, appeal, or adjudication. The information gathered by the AO should be reported to the CAC and be maintained with provider anonymity to ensure that auditor’s recommendations are reliable, valid, and useful. CAC reports can be appealed to the CAC based on a second opinion provided by a qualified independent Certified Internal Auditor (CIA). Final appeal would be the using a State sponsored arbitration process.
The Audit Officer’s (AO) function is to oversee, prioritize, educate and mitigate when possible, the clinical, ethical, legal, compliance, regulatory, financial, and other risks to Healthplan Operations and Provider Practices. The AO works with the CAC to implement policies and practices that prevent risks impacting objective caused by a lack of transparency and clarity from becoming manifest. In addition, the AO provides education, counsel, and support to the CAC on legal, audit, compliance, and risk matters created by Healthplans and/or provider practices. The AO also works to develop and model a culture that supports and encourages adherence with applicable laws and regulatory codes of conduct and ethical principles with transparency in assigned personal and business dealings and demonstration of integrity and respect in all interactions.
The AO will assess and make recommendations for “controls” and “test scripts” (i.e., contract management and monitoring scripts) based on an analysis of existing or proposed contract changes and contract requirements as they affect shared values, objectives, controls, scripts, and key performance indicators. The AO also will have the ability to identify values and objectives, and recommend “controls”, “scripts”, and key performance indicators that (1) value diversity, (2) audit issues for a range of sub-populations, (3) make recommendations that recognize the dynamics of difference, (4) acquire and incorporate cultural knowledge and human differences, and (5) adapt to diversity and the cultural contexts of provider practices who work with populations who are marginalized or otherwise underserved.
Discussion of One Healthplan’s Contract Proposal
In October 2022, one Healthplan (Healthplan X) offered and implemented a new contract for groups in their provider network. The framework of that contract implements some elements of the Centers for Medicare and Medicaid that trend toward rate reductions annually but left out the regional Geographic Practice Cost Index. The CMS rates are arguably low and not competitive. The rate was initially less than CMS for counselors, LMFTs and Licensed clinical social workers. (Lower than what they would be paid contracting with Medicare.) Healthplan X also offered provider practices a Behavioral Health Incentive Program (BHIP).
The contract offered was in effect, take-it-or-leave-it (i.e., a contract of adhesion). Problems surfaced. For example, in a quality improvement initiative, provider practices, as well as providers and Healthplans, must be allowed to communicate and work together to establish common values, objectives, goals, measures, strategies, technology, information, public health concerns, and special population needs. Healthplan X refused to reveal the identity of provider groups sharing risk in a value-based payment contract. Groups sharing risk must be able to communicate in order to be able to achieve targets.
OHA, HPC-LAN and ORCompact lead providers to define value as (1) evidence-based, (2) patient-centered, and focused on (3) improved quality and positive health outcomes at appropriate cost. Rather than creating contracts by “making it up as we go” as Healthplan X stated they are doing, there must be an explicit process to monitor, manage and control risk, and to adjust the risk, so that neither Healthplans nor Providers fail because they were acting in good faith relying on framework that was undefined or ill-defined, and not agreed on. Good faith agreement requires transparency of anything that is “material” and necessary for both parties to succeed.
The OHA recommends a stepwise ladder approach to adopting VBP contracts. There are a series of steps (See Table 1.) Healthplan X has offered a contract that skips category 2 and begins with Category 3. Healthplan X is enticing providers practices to begin contracting as if they are category 3 capable. It is probable to almost certain that provider practices are not category 3 capable. And they don’t know what they are skipping. The benefit to Healthplan X is that by skipping category 3, they can avoid investing in the necessary technology, and still demonstrate to healthcare purchasers that they are adopting VBP as required by the ORCompact, but to the detriment of providers who are likely to fail within the next 3 years. (See Figure 2. Unacceptable Value-Based Payment Contract.)
Table 1. Learning Action Network Stepwise Ladder to Adopt VBP.

Objectives such as profit, reducing costs, and administrative burdens can impact other objectives such as patient access, coordination of care, measurement, provider satisfaction with the contact, etc. Objectives of a Healthplan, especially objectives which are not transparent, can in fact be a risk or threat to provider practices’ achievement of targets. Low trust in partnering with Healthplans is the result of Healthplans’ history of bad faith contracts, unfair practices, and provider dissatisfaction because their concerns for patient well-being are ignored. This leads to contract “gaming”, such as reducing providers’ case-mix severity, or to dropping out of contracts. “Phantom networks” are created when Healthplans maintain lists of provider practices that have either terminated or are preparing to terminate their contract, seeing very few or no patients. The effect is reduced access to care. If providers practices and Healthplans are not able to align on shared values, objectives, controls, test scripts and key performance indicators, Healthplans and providers cannot effectively manage the risks that impact them both.
In the case where Healthplans focus on “waste” as an objective, providers may conclude the Healthplan’s objectives and controls are unfair; especially if the effect of a contract generates profits by not providing care and increases provider practices’ risk and liability. The framework of VBP contracts must have “controls”, test scripts and key performance indicator which can be used to manage upside risk and/or downside risks in ways that are fair and implemented in good faith. For example, upside risk for Healthplans' will result when Healthplans design contracts to their benefit (i.e., favorable risk of meeting their targets). The downside risk for provider practices will result when Healthplans design the contract to the detriment of provider practice and patient health (i.e., probable to almost certain risk of failure to meet provider practices targets). Healthplan X provides examples of what not to do when offering a contract to provider practices.
Contracting Framework for Ethical and Effective Contracting with Mental & Behavioral Health Practices
Oregon has long been a national leader in health system transformation, focused on creating systems for delivering affordable, high value coordinated quality care. In 2019, the legislature created the Sustainable Health Care Cost Growth Target implementation Committee and charged it with identifying mechanisms to lower the growth of healthcare spending to a financially sustainable rate. In October 2020, the Implementation Committee for the Oregon Value-Based Payment Compact created a set of principles to increase the spread of value-based payment (VBP) models across the state as a strategy to improve quality and lower costs, and recommended that payers, providers, and other stakeholders across the state make a voluntary commitment to participate in and spread VBPs.
The cost of health care in Oregon has grown and is projected to grow faster than both the state economy and Oregonians’ wages. The health care cost growth target is a target for the annual per capita rate of growth of total health care spending in the state. Cost increases of health insurance companies and health care provider organizations will be compared to the growth target each year. The program will also evaluate and annually report on cost increases and drivers of health care costs. The voluntary allowable increase target is 3.49%.
Converting their contracts to Medicare reimbursement rates, Healthplan X’s strategy had the impact of reducing provider rates within 2 months of providers signing that contract in November 2022. An outpouring of anger from providers who believe they were misled, coupled with Healthplan X telling a provider group practice that they did not know this would happen, subsequently resulted in Healthplan X increasing provider practices reimbursement rate on or about April of 2023. The manner in which Healthplan X increased their rates is not aligned with the framework of Medicare’s reimbursement calculation. Healthplan X increase was not proportional to Medicare and was less favorable to psychologists, and especially to social workers and counselors. (See Table 3. Display of Hidden Systematic Benefit to Healthplans to the Detriment of Unwitting Provider Practices.)
Healthplan X also adopted the Medicare conversion factor and left out the Geographic Practice Cost Index and the CPT code Relative Value Units (RVU) necessary to create baselines, a systematic benefit to Healthplan X (i.e., a Healthplan saving of approximately 11%). Providers were not adequately informed by Healthplan X and this led providers to make decisions they would not have made had they been fully informed.
Table 2 and Table 3 illustrate the systematic benefit to Heathplan X over Unwitting Provider Practices. These tables provide information that providers who have no experience with Medicare Conversion Factors, Relative Value Units, and Geographic Practice Cost Index, and their interactions over time with inflation and Medicare Economic Index. Relying on the Medicare Conversion Factor would be substantially more than a declining 2023 and 2024 Healthplan Multiplier.
Table 2. Projected Reductions in CMS rates from year 2020 to 2025.
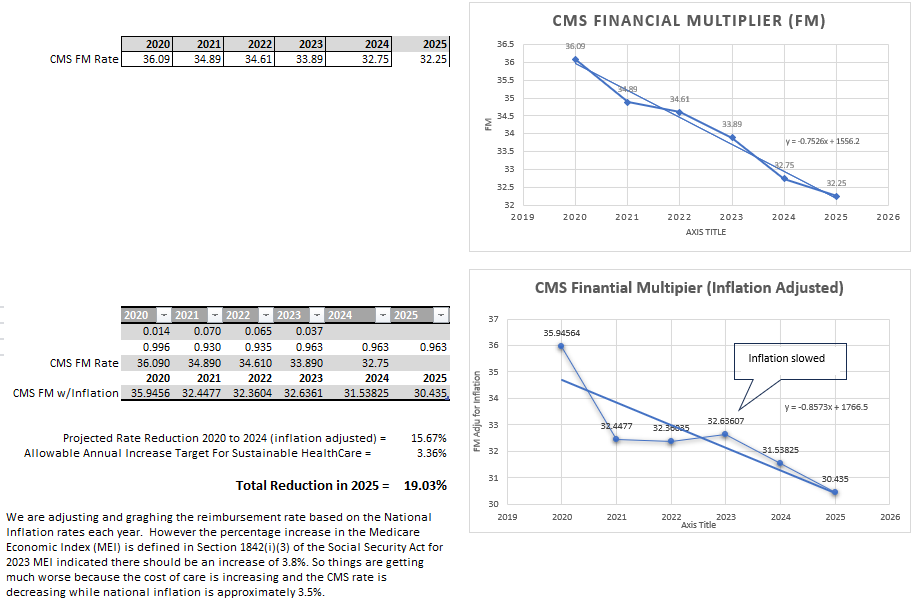
Table 3. Display of Hidden Systematic Benefit to Healthplans to the Detriment of Unwitting Provider Practices.

Subsequently, a provider practice group confronted Healthplan X, negotiated, and made assurance to a contracting group that rates would not drop in 2024. Healthplan X rescinded their assurance months later without telling the contract negotiator. Again, providers were misled. When confronted, Healthplan X stated they were assessing whether or not they will allow the expected automatic rate reduction to go into effect until 2024. Providers must wait and see whether or not rates will drop in 2024. This will require provider practices to continue to see patients for 120 days before they can drop their contracts. These are just a few examples of bad faith and unfair dealing out of a list of 42 that demonstrate bad faith and unfair dealing in contracts which are toxic to providers services and undermine public health and trust. At that point the provider group negotiating with Healthplan X consulted with a Certified Internal Auditor and Compliance Officer for a reputable hospital, physician, mental health, and behavioral health network.
In Oregon, there are a many significant challenges in the delivery of mental and behavioral health and substance use treatment services related to supply and demand factors. Specifically, demand is greater than the supply of qualified professionals to meet the demand, which has led the State of Oregon’s legislators to pass legislation to address the importance of assuring mental health parity. Healthplans have not been responsive to Senate Bill 860 and there are questions whether the parity objective of access to care is being supported by Healthplans. Some Healthplans have responded by increasing amounts paid for various mental health services while other Healthplans have sought to established “narrow networks with incentives” to attend to the mental health needs of plan members. Other Healthplans have taken a “wait and see” approach, watching where the industry goes and whether programs such as integrated care models increase access through primary care settings.
The OHA Healthcare Sustainable Growth Target Program has recently focused on “What is happening with behavioral health spending?” Despite two decades of research and guidance from provider associations, research institutions, industry thought leaders and consultants, Oregon Healthplans have not implemented quality improvement programs for mental and behavioral health services using Fee-For-Service (FFS), Alternative Payment Methods (APM) or Value-Based Payments (VBP). At best, they have implemented utilization limitation controls (e.g., audits of factors that are not material to the Oregon Health Authority values and objectives). Healthplans are creating administrative burdens that alienate and intimidate provider practices intimating these are necessary new contact requirement in their quality improvement programs.
In a quality improvement initiative, providers, as well as providers and payers, must be allowed to communicate and work together to establish common values, objectives, goals, measures, strategies, technology, actionable information, public health concerns, and special population needs. This cannot be presumed and dictated as shared values unless Healthplans and providers work as partners. Partnering requires open and transparent conversations. Healthplan X is not demonstrating good faith and fair dealings which are necessary to enter into a value-based payment agreement/partnership.
To partner responsibly in a value-based payment contract, providers and Healthplans must define and develop shared values, shared objectives, transparent “controls” and key performance indicators based on criteria for their achievement. These cannot be dictated and offered as a value-based payment contract especially if provider practices are not provided the information and resources, they need to evaluate the contract.
Providers and Healthplans need to define the values and objectives which ethically and clinically require what are necessary or expected as deliverable services. Controls must protect the ethical requirements incumbent on mental and behavioral health professionals. These should be transparent and shared with all provider groups, independent providers, and Healthplans. If this does not happen, the contact becomes a “game of chance” with Healthplans that has a “stacked deck”.
Contracting requires conversations as illustrated in Figure 1. Conversations are essential if provider practices wish to avoid “games of chance” using contract language stacked against provider practices.
Figure 1. Conversations for Successful Contracting.

Review of Oregon Health Authority (OHA), Health and Human Services Health Payer Center Learning Action Network (HPC-LAN) and Oregon Value-Based Payment Compact (ORCompact) documents lead to definitions of value as (1) evidence based, (2) patient-centered, and focused on (3) improved quality and health outcomes at an appropriate cost. Those values are not deliverables. Actions including screening, symptom, progress and outcome measures, and coordinating care are examples of deliverables. Deliverables can be measured. Deliverables require baselines and benchmarks, infrastructure, processes, and outcome measurement processes. Deliverables cannot be dictated by payers’ requirements that providers must invest time and money to create processes that are not defined, measurable or achievable. The population of patients in Oregon has too many sub populations for a one-size fits all approach. Some populations require more resources (i.e., time, skill, services) than others. Culturally appropriate and special needs services are necessary and require training and specialization.
Value-based payments are not designed, negotiated, or evaluated in the same way as fee-for-service contracts because P4P, APM and VBP contracts involve risk and risk sharing among providers and often Healthplans. VBP contracts and APMs are developed and adjusted over time because there must be risk-adjustments for technology, analytics, sub-populations and changes in the defined values and objectives. Managing changes requires the use of agreed upon “controls.” Controls are important factors. Nationally, providers and Healthplans struggle to implement controls in a transparent manner. Historically, Healthplans maintain control using Contracts of Adhesion (i.e., take it or leave it), and processes known only to the Healthplan (that can be viewed by providers as arbitrary and capricious).
If a Healthplan’s model for VBP contracting is to “make it up as we go”, this will create an additional degree of risks that will impact objectives, if not immediately, almost certainly over a 3-year period. Rather than “make it up as we go”, there must be processes to monitor, manage, and control risk, and to adjust the risk, so that neither Healthplans nor Providers fail when they act in good faith using an untested contract. A poorly designed contract of adhesion can be unmanageable, inequitable, and cannot be changed or re-negotiated when problems are revealed. The LAN Stepwise ladder to adopt VBP should be followed (see Table 1. Learning Action Network Stepwise Ladder to Adopt VBP.)
Based on surveys as far back as 2015, mental health providers opine that their contracts are designed by Healthplans to benefit Healthplans, to the detriment of providers’ practices, and to patients’ health. This happens when Healthplans do not define and share all their objectives, and instead assume that providers’ objectives are aligned with Healthplan’s, and subsequently audit providers’ compliance based on the Healthplan’s objectives.
The cultures of Healthplans and providers have similar and different priorities. Healthplans prioritize employer marketing, employer satisfaction, employee health, etc. Providers prioritize appropriate referral channels, support services, billing technology, patient care, ethical practice, a balance in patient case mix severity, liability, patient risk and health.
It is important to analyze how Healthplan objectives and provider objectives impact each other. For example, objectives such as profit, reducing costs, and administrative burden can impact other objectives such as patient access, coordination of care, provider satisfaction with the contact, etc. Low provider satisfaction can lead to providers gaming or dropping contracts. In the case where Healthplans focus on “waste” as an objective, providers conclude the Healthplan’s objectives and controls are unfair; especially if the effect of a contract generates profits by not providing care. If providers and Healthplans are not able to align on common objectives, then Healthplans and providers cannot effectively manage the risks that impact them both. The framework of VBP contracts must have controls to manage upside risk and/or downside risks in ways that are fair and created in good faith.
Figure 2. Unacceptable Value-Based Payment Contract.

Figure 2 is a visual analysis of risks and consequences. The bubbles are inherent and explicit risk-impacting-objectives. This heatmap displays visually the inherent risks of a contract if nothing is changed. The bubbles can be used to facilitate a discussion of the interacting effects of values, objectives, and controls.
MRI and IMHPA’s interpretation of Figure 2 is that the Healthplan X Master Agreement and the BHIP should be re-designed. The distribution of the bubbles illustrates that the inherent risks benefit Healthplan X with a strong upside risk over a significant downside risk over time for participating providers. Impacts on providers will surface immediately and within year 1 and the remaining impacts within 3 years. There are probable to almost certain moderate to catastrophic consequences to participating provider and public health objectives. Left unchanged, the framework of this contract has significant risk or no value to providers, patients, and public health. Healthplan X was unwilling to discuss or respond to written questions required to implement controls such that the risk would not map from yellow to red. Value-based contracting is feasible if the risks impacting objectives are in the green, which would be a healthy contract, one that will benefit providers, the Healthplan, and public health.
The most important question facing providers is whether a contract is fair, made in good faith, and is manageable. Using the presented Top Risk Review Heatmap allows providers and Healthplans to ascertain risks, the value, and the requirements of a contract moving forward before the contract is offered or signed. Figure 1 demonstrates visually that Healthplan X and provider practices in Oregon are not aligned. In this case, this misalignment is to benefit of Healthplan X and systematically to the detriment to all provider practices and public health.
In practice, risk is assumed by a Healthplan, among providers, or shared between providers and the Healthplan. Absence of dedicated effort to partner suggests that a Healthplan does not want to share risk with providers. Healthplan X’s current contracting method requires providers to assume an unfair level of risk and benefit immediately and over time. This risk relationship illustrated in Figure 3 is asymmetric.
For example, absent assurance, a Healthplan may subsequently conduct an audit for compliance, instead of an audit that supports quality improvement of services that will achieve targets. Providers are not willing to assume any additional risk especially when Healthplans create “controls” that are not transparent and not negotiable. By not partnering, FFS, APM and VBP contracts for mental and behavioral health services can lead to gaming.
Figure 3. Asymmetric Risk-Benefit for Healthplan X and Provider Practices.

Figure 3 illustrates the risk and benefit dynamic of Heathplan X’s effort to attract provider practices to sign a seemingly innocuous contract that offers a “false profit leader” an incentive that has no explicit risk and no expectation to deliver anything and you get paid more (i.e., “Just measure anything”). A false profit leader is the opposite of a “loss leader.” Loss leaders are widely considered predatory business practice, drawing customers in for a low cost only to upsell another product that costs more because the original product is no longer available. A false profit leader draws provider practices in to sign agreements for what appears to be a profit. The profit may not be proportional to the cost of changing requirements, or provider practices do not have the resources to perform a Test of Design or Test of Effectiveness. But signing the contract has value to a Healthplan attempting to implement a value-based payment program. Signing the contract endorses Healthplan X, improves their brand recognition in the market, and allows them to meet ORCompact requirements.
Healthplan X’s false profit leader for their contract seemingly has profit, but it has no measurable value, nor are there scripts (e.g., instructions) that an Auditor can use to verify how incentives are related to tasks. The systematic benefit to Healthplans which is to the detriment of providers and the public is “rigged” to gather support for the contract (i.e., gaining face value to plan purchasers) rather than support for a contract based on shared values that have actual measurable value (i.e., shared value). Once signed, from that point forward, the Healthplan almost certainly can control providers’ practices. Provider practices do have the choice to leave the contract after the experience of having sacrificed their opportunity costs while altering their practice to adjust to the Healthplan’s requirements and policies. Policies that should have been transparent to begin with and not made up by Healthplan X as they see fit.
Providers entering a contract of adhesion are unwittingly vulnerable, they are given no assurance otherwise, and can expect with near certainty that Healthplan X will switch requirements to achieve more difficult targets. Healthplan X is bypassing recommendations for setting baselines from which benchmarks (i.e., targets) can be achieved. Without baselines and reasonable benchmarks, Healthplan X’s underlying framework will almost certainly benefit the Healthplans (i.e., low risk, high benefit) to the detriment of providers (i.e., high risk of failure, low benefit, or a loss).
National Committee for Quality Assurance (NCQA) standards are a roadmap for improvement. Healthplans use these roadmaps to perform a gap analysis and align improvement activities with areas that are most important to State governments and employers, such as network adequacy and consumer protection. NCQA Standards evaluate plans on:
Quality Management and Improvement.
Population Health Management.
Network Management.
Utilization Management.
Credentialing and Recredentialing.
Members’ Rights and Responsibilities.
Member Connections.
Medicaid Benefits and Services.
According to NCQA, the use of Healthcare Effectiveness Data and Information Set (HEDIS) data allows the Health Plan Accreditation process to effectively measure care and service performance. This focuses attention on activities that keep members healthy.
NCQA does not provide useful guidance for value-based payment contracting for psychiatric, psychotherapeutic, or counseling services. Guidance for contracting is provided by provider organizations, thought leaders, industry expert consultants, professional associations, the Department of Health and Human Services, and the Oregon Health Authority.
Why is independent auditing so important?
Objectives for VBP contracts have been widely published. Mentor Research Institute (MRI), working with a certified auditor and compliance officer, selected 18 objectives that should be inherent in the proposed Healthplan X Healthplan contract. A Risk Impacting Objectives (RIO) and Risk Control Matric (RCM and a Heatmap was created. After reviewing contracts of other Healthplans, MRI identified 3 more objectives. Contracting groups need to know Healthplan X’s values and objectives and to have those stated in ways that can be defined, shared, measured, and used to set baselines and benchmarks for which quality improvement targets can be defined. To do otherwise is not an appropriate or responsible business practice. Independent practice providers and group practice providers need to know as well. For example, is it the objective of Healthplan X to support independent practice or to fold independent practice into employer owned groups? That declaration, one way or another, is an objective or risk that interacts with other objectives. This is natural consequence if Healthplan draws group practices into their BHIP, however, the misalignment of objectives will erode the relationship between the Healthplan and provider practices. All the waste, as Healthplans and provider practices game the contract could have been avoided.
Quality care has been categorized by the American Psychological Association (APA) as infrastructure, processes, and/or outcomes. Improvements in quality must be measured, correlated with shared values and objectives, and be reimbursed at an appropriate rate. Healthplan X has not identified any objectives we are aware of that align with APA, OHA, the ORCompact discussions, or with providers’ core values and established standards for delivery of ethical clinical services.
Measurement-Based Care and (MBC) and pay-for-performance (P4P) are necessary steps before alternative payment methods (APM) and VBPs are instituted. Risk-sharing cannot take place in the absence of the ability to establish baselines and recognition of the necessity of investment in needed infrastructure, processes (standards of practice), and outcomes incentives.
Value-based payments are not designed, negotiated, or evaluated the same way as fee-for-service contracts because P4P, APM and VBP contracts involve risk and risk sharing among providers. Healthplans do not want to invest in the necessary changes to implement P4P, APM and VBP . VBP and APM contracts are complicated as time passes because there must be risk-adjustments for technology, analytics, sub-populations, and changes in prior definitions of values and objectives. Managing changes requires management using agreed upon controls. Controls are important factors which providers and Healthplans struggle nationally to implement in a transparent manner. Historically, Healthplans maintain control using contracts of adhesion (i.e., take it or leave it), and policies that are hidden, arbitrary and capricious.
For more information see:
https://www.mentorresearch.org/pacific-source-26-appointments-audit
It is important to analyze how Healthplan objectives and provider objectives will have an impact on each other. If providers and Healthplans are not able to align on common objectives, then payers and providers cannot effectively manage the risks that impact them both. The framework of VBP contracts must have controls to manage upside risk and/or downside risks in ways that are fair and are created in good faith.
Because there are no shared objectives, the risk and benefit in the Healthplan X master agreement and BHIP framework will benefit Healthplan X with a high upside risk. The downside risk has moderate to almost certain consequences to providers’ ability to achieve shared objectives now or in the future. Providers must be allowed to examine and comment on the controls, test scripts, and updated scripts that will be used to evaluate the contract. For example, providers should seek a contact assurance that the contract audit involves a transparent Test of Design (TOD), Test of Effectiveness (TOE), and a heatmap.
The shared Purposes and Rationale (Figure 4) suggested by Healthplan X cannot be used to measure value and achievement of objectives in a reliable, valid and useful manner. Unless providers and Healthplans can construct a contract, which group and individual practices can understand and know is fair, and made in good faith, MRI is certain that providers will find evidence to reach harsh conclusions. Conclusions, which MRI is already hearing from informal conversation, will be difficult to control and undo in the era of social media. MRI wants Healthplan X and provider practices to succeed. The odds of that happening are low as illustrated in Figure 2. The fact that Healthplan X does not want to understand and discuss Figure 1 is the most likely conclusion because Healthplan X does not wish to discuss provider practice concerns and has yet to respond to provider letter and emails.
Healthplan X’s BHIP contract is vulnerable to misunderstanding because of its need for greater specification, and numerous errors of omission and commission. For example, the purpose and rationale Healthplan X has provided is a combination of goals, requirements, and methods (Figure 4). While there are indeed shared beliefs, these are not values, nor are they objectives that can be measured as such. Healthplan X uses the word incentive which providers will consider synonymous with value-based payment. Healthplan X’s use of the word “options” is synonymous with sub agreements within a base contract (i.e., the master service agreement).
Figure 4. Quoted from the Healthplan X Contract
1. Purpose and rationale
The Healthplan X Behavioral Health Incentive Program (BHIP) is an opt-in program designed to support providers’ delivery of quality of care. It is a combination pay-for-participation and pay-for-performance model, meaning that all behavioral health organizations who opt in and participate in the elements of the model will receive an incentive. Additionally, if Healthplan X’s overall performance target is achieved then an additional bonus will be added. The program is based on the following shared beliefs:
1.1 Member health and welfare is at the center of our work and our outlook in securing effective care.
1.2 Our providers are our primary means of delivering quality of care and building on that relationship will directly enhance all involved.
1.3 Coordinated and collaborative care enhances our members’ ability to access care readily, timely, and easily.
1.4 The adoption of evidence-based practices can improve outcomes. Extensive research supports the effectiveness of treatment which attends to the member’s voice by systematically inviting member feedback on the process of care and member-reported outcomes (Feedback Informed Care [FICare] or Feedback Informed Treatment [FIT], also variously known as Patient-Reported Outcome Measures [PROMs], Outcome Informed Care [OIC], Measurement Based Care [MBC], etc.)
1.5 Such data collection is pan-theoretical and can readily be incorporated into a wide variety of provider practices, treatment modalities and clinical paradigms.
[Note: There little to no evidence that “1.3 Coordinated and collaborative care enhances our members’ ability to access care readily, timely, and easily.”]
Providers are highly concerned about the variety and impact of differing payer requirements and audit procedures that have no discernible value, no shared objectives, are not fair nor negotiated in good faith. These differing requirements make it difficult to manage practices across multiple-payer contracts. These are risks that will impact crucial objectives such as patient access. There must be controls to manage payers’ contract changes and their cumulative impact across multiple payers (i.e., many contracts will add and change requirements over time, and so will the risks.)
A “false profit leader” is the opposite of a “loss leader.” (Loss leaders are widely disapproved as predatory, drawing customers in for a low cost only to upsell another product that costs more because the original product is no longer available.) Attracting provider practices to sign a seemingly innocuous contract offering an incentive that has no risk, and then switching requirements to achieve incentives that have a risk framework to benefits a Healthplan to the detriment of providers is a false-profit tactic. A false profit offer draws provider practices to sign agreements for profits that are “rigged” to gather agreement (i.e., face value), that will appear valuable to employers who purchase Healthplans for their employees, and are likely to be changed in ways that further benefit the Healthplan to the detriment of provider practices.
Healthplans should not want their contracts to be viewed as a “bait and switch.” Bait and switch in this context means that there are missing agreements, assurances of requirements in the contract a Healthplan intends to add during the contract cycle management. This a problem if one wants to protect public health because a “bait and switch” precedent used in one Healthplan contract may be expected in another Healthplan’s contract with the declaration that “other Healthplans do this as standard practice.” The problem for providers is that Healthplans can implement requirements which have differing administrative demands, measurements, values, objectives, required technology, and costs. This is happening across several Healthplans with cumulative impacts on providers. Providers will become overwhelmed with contracts that are not unified, strategic and differ in their requirements.
The Healthplan X contract is based on ‘asymmetric information” that benefits Healthplan X and makes providers unable to ascertain the current purpose or future value of contracting with Healthplan X. The framework is not defined. The contract does not have the necessary language that could support APM and VBP. It sets up provider practices, not the Healthplan, to fail.
The Healthplan X contract is a contract of adhesion (i.e., take-it-or-leave-it).
The Healthplan contract has a “false profit” incentive that entices provider practices to sign a contract that has a moderate to almost certain risk of harm and failure.
The Healthplan X contract leverages all risk and benefit to Healthplan X to the detriment of contracted providers.
The Healthplan X contract is almost certainly a waste of taxpayer and employer money.
The Healthplan X contract has no defined shared values.
The Healthplan X contract has no defined shared objectives.
The Healthplan X contract has no defined target related to incentive reimbursements.
The Healthplan X contract has no clear or shared purposes.
The Healthplan X contract has no shared strategies.
The Healthplan X contract has no targets providers have an ability to achieve.
The Healthplan X contract has no provider shared risks with Healthplan X.
The Healthplan X contract has no risk adjustment process for special populations.
The Healthplan X contract was almost certainly created in bad faith with unfair risk.
The Healthplan X contract is almost certainly a waste of provider resources given the opportunity cost.
The Healthplan X contract has no contract cycle management.
The inherent risk in the Healthplan X contract, moving forward, is a probable to almost certain risk of moderate to catastrophic impact on Provider practices, public health, and the credibility of value-based contracting for mental health services.
Providers are unable to manage multiple VBP contracts, each with unique quality improvement programs.
The Healthplan X contract is almost certainly flawed to such an extent that the entire contract cannot be reliably audited and is almost certainly unenforceable.
Healthplan X is unwilling to have conversations, be transparent and expects provider practices to give Healthplans a high upside risk while providers practice assume a high downside risk.
Historically, and unfortunately, the relationship between payers and providers has been challenging, sometimes adversarial. To partner, there must be an independent source of information to help providers and payers govern contracts. MRI has identified a solution that will be fair, accountable, patient centered, that will support and develop quality improvements at appropriate cost. This solution is a standard in organizations such as a hospital-physician-and allied health systems of care that employ internal auditors: Independent audit of contracts before providers or provider groups sign them.
Healthplans and providers need resources that offer qualified, objective, impartial information that can be used to determine if there are reliable and valid contract requirements and reimbursements for their practice. The challenges facing VBP contracts between Healthplans and providers can be resolved if Healthplans, who create changes in contract or new contracts, have their contracts audited by an independent contract auditor before and during the implementation of new contracts or changes in contracts. This is a standard process for hospital physician networks that contract to protect the public. Payer contract audits must be public and consider public input.
“Contract auditing” means an independent, objective assurance and consulting activity is required of both payers and providers, a process designed to add value, create and meet shared objectives, improve contracted operations and effectively manage contract cycles. The purpose is to ensure transparency and data informed decisions that are evidence-based, patient centered, and that support improvements in quality at an appropriate cost.
The auditor will help providers and payers identify shared values and to accomplish their shared objectives by bringing a systematic, disciplined approach to evaluate, and improve the contract effectiveness of risk management, controls, and their respective governance processes.
Independent contract auditing will achieve this goal by gathering, aggregating, and analyzing data providing information, insight and recommendations based on analyses and assessments of data and contracted business processes.
Excerpts from measurement-based care (MBC) proposals from AMHA-OR (now IMHPA) to Healthplan X
AMHA-OR is an incorporated member-owned group practice whereby psychotherapists may opt in or out of contracts.
Members of AMHA-OR are trained to use the LightQ EHR and measurement platform and they present their practice information in the therapist locator at OregonTherapyOptions.com.
Providers will be asked to obtain mutually agreed on screening, progress, and satisfaction measures as they provide services.
Providers will document that people seeking care were offered an appointment in a timely manner.
Psychotherapist members of AMHA-OR should be reimbursed a fixed amount per screening for their time and technology use. Using uniquely identifiable CPT codes (e.g., 90899, 90785) will (a) avoid unnecessary provider costs, (b) reinforce appropriate administration, (c) reduce error in subsequent analysis, (d) reduce expense to the contracting organization (i.e., Healthplan), (e) eliminate the appearance of fraud, and (f) allow providers to conduct relative value analyses. The 90785 CPT code will allow providers to set baselines and to calculate adjustments in reimbursement for patients when there is need to work with parents, family members and/or to coordinate care with physicians and assisted care providers.
MRI recommends Healthplan X collaborate with AMHA-OR to include Associate Licensed Counselors, who have AMHA-OR member supervisors (certified by the State of Oregon) in the Healthplan X contract. This will increase the number of available appointments to Healthplan X members seeking services by an estimated 93% (+/- 37%) in the first year. A Healthplan X access initiative is permissible in the State of Oregon with licensed professional and AMHA-OR oversight. The AMHA-OR Board will assume administrative responsibility for the program, ensure there is qualified clinical supervision, and enforce program policies; supervising supervisors, and auditing Associate Licensed Counselor members of AMHA to ensure medical necessity of care, that standards for documentation are followed, and that treatment is empirically supported.
If Healthplan X agrees to the essentials for ethical practice, business operations and MBC, psychotherapist members of AMHA will opt-in depending on the reimbursement rate. AMHA-OR member dues are being used to create and administer contracts. Psychotherapy services will be reimbursed at a rate calculated by using a Healthplan X multiplier for which the product of the CMS rate is no less than the Oregon Health Plan (OHP) rate for CPT® 90834 code: Psychotherapy, 45 Minutes. MRI estimates this to be a minimum competitive rate for private practice adoption of MBC. The 90834 is the most frequently used CPT code and that rate, more than other codes, determines the willingness of a provider to see complex and urgent cases.
Healthplan X Health will fix the reimbursement rate set by CMS and apply the annual allowable increase set forth by the OHA and ORCompact.
The decision to shift priorities and workflow between appointments from a focus on charting and treatment to measurement technology requires (a) work and (b) practice efficiency/expense, and (c) must be rewarding. The reward must be timely and paired closely to a new task (i.e., target behavior). A financial incentive for deliberate practice and the anticipation of gaining information that is useful is rewarding. It is also respectful of psychotherapists’ time, memorable, ethical and a buffer against the distressing experiences and chronic conditions that psychotherapists encounter in their work. A fixed ratio reinforcement schedule of 1 is the most effective way to change choice behavior; and overcome providers’ resistance to MBC, OIC and FIT.
Issues and Requirements for Successful Fee-For-Service, Pay for Performance, Measurement-Based Care, Alternative Payment Methods and Value-Based Payment Contracting
In January 2022, MRI responded to a Healthplan X Health’s request for proposals (RFP). MRI offered a program that incorporated relevant implementation science research. The program addressed:
A provider and patient centered approach.
Measurement/instrument agnostic (patient and provider centric).
Quality improvement at appropriate provider compensation.
A technology platform that gathers, aggregates, analyzes and information reporting that offers ease of use.
Training and support which must be ongoing.
In October 2022, Healthplan X offered and implemented a new contract for their provider network. The framework of that contract implements some elements of the Centers for Medicare and Medicaid that trend toward rate reductions annually but left out the regional Geographic Practice Cost Index (GPCI). The CMS rates are arguably low and not competitive. Leaving out the CMS GPCI saved the Healthplan 3 to 5 million dollars. The reimbursement rate was initially less than CMS for licensed professional counselors (LPC), licensed marriage and family therapists (LMFT) and licensed clinical social workers (LCSW). Lower than what they would be paid if they accepted Medicare. Healthplan X also offered providers their Behavioral Health Incentive Program (BHIP).
In a quality improvement initiative, providers, as well as providers and Healthplans, must be allowed to have conversations and work together to establish common values, objectives, goals, measures, strategies, technology, information, public health concerns, and special population needs. Healthplan X refused to support this. OHA, HPS-LAN and ORCompact lead providers to define value as (1) evidence-based, (2) patient-centered, and focused on (3) improved quality and positive health outcomes at appropriate cost. To accomplish this, Healthplans and Provider Groups need to have conversations. Rather than creating contracts by “making it up as we go”, there must be a explicit processes to monitor, manage and control risk, and to adjust the risk, so that neither Healthplans nor Providers fail when they act in good faith relying on an contract that could be ill-defined. Objectives such as profit, reducing costs, and increasing administrative burdens can impact other objectives such as patient access, coordination of care, measurement, provider satisfaction with the contract, etc.
Low trust in Healthplans, is the result of bad faith contracts, unfair practices, and provider dissatisfaction. This leads to contract “gaming”. For example, providers can resort to minimizing their case-mix severity to save time, not accepting new patients, or to dropping out of contracts. If providers and Healthplans are not able to align on shared values and objectives, Healthplans and providers cannot effectively manage untorrid risks that impact them both.
In the case where Healthplans focus on reducing “waste” as an objective, providers may conclude the Healthplan’s values, objectives and controls are unfair; especially if the effect of a contract generates profits by not providing care, and increases provider practices liability and risk. The framework of FFS, APM or VBP contracts must have “controls” which can be used to manage upside risk and/or downside risks in ways that are fair and are created in good faith. Controls include procedures to hold Healthplans accountable to using audit procedures in ways that have mutually agreed on values and objectives.
Practice Structures for Fee-For-Service, Alternative-Payment Methods, and Value-Based Payments
Independent mental and behavioral health provider practices take 3 forms:
A licensed clinician working solo (incorporated or not).
A group of licensed clinicians sharing the expenses of space, staff, billing services, etc., with informal agreements.
An incorporated practice group where the expenses of practice are shared on a formal basis, and malpractice and general liability insurance involve shared coverage (using a shared Tax ID and NPI).
Independent practices can incorporate to contract together as Independent Practice Associations (IPAs) that are member owned.
Mental and behavioral health practice that is not “independent” also takes 3 forms and is growing rapidly:
Professionals employed in medical facilities or health agencies.
Professionals employed in groups with salary and benefits.
Professionals employed in groups on a 1099 contract basis.
Contracts structured for FFS, APM and VBP for mental and behavioral health services must align with the values and purposes common to the professionals working in each of these structures.
References
Aafjes-Van Doorn, K. & de Jong. K (2022). “How to make the most of routine outcome monitoring (ROM): A multitude of clinical decisions and nuances to consider.” Journal of Clinical Psychology 78(1)s
Britton, T. (2022) “Value-based Care in Addiction Treatment: Why it’s Essential and How we get There.” Addiction Professional, October 18, 2022.
Duncan, B.L., & Reese, R.J., (2015). The partners for Change Outcome Management System (PCOMS): Revisiting the client’s frame of reference. Psychotherapy, 52:4, 391-401.
Guo, T, et al (2015) Measurement-based care versus standard care for major depression: A randomized control trial with blind raters. American Journal of Psychiatry, 172:10, 1004-1013.
Howard, K., C., Davidson, C., O'Mahaney, M., Orlinsky, D. & Brown, K. (1989) "Patters of Psychotherapy Utilization." American Journal of Psychiatry.
Howard, K., Kopta, Krause, M., & Orlinsku, D. (1986). "The Dose-Effect Relationship in Psychotherapy." American Psychologist 41(2).
Kadera, S., Lambert, M., & Andrews, A. (1996).. “How much Therapy is Really Enough?” Journal of Psychotherapy Practice and Research.
Kopta, M., Owen, J., & Budge, S. (2015). Measuring psychotherapy outcomes with the behavioral health measure-20: Efficient and comprehensive. Psychotherapy, 52:4, 442-448.
Lambert, M.J. (2015). Progress feedback and the OQ-System: The past and the future. Psychotherapy, 52, 381-390.
Lewis, C. C, Scott, K., Marti, C.N., Marriott, B.R., Kroenke, K., Putz, J.W., Mendel, P., & Rutkowski (2015). Implementing measurement-based care (iMBC) for depression in community mental health: A dynamic cluster randomized trial study protocol. Implementation Science, 10:127.
Lewis, C.L., Boyd, M., Puspitasari, A., Navarro, E., Howard J., Kassab, H., Hoffman, M., Scott, K., Lyon, A., Douglas, S., Simon, G., & Kroenke, K. (2018). Implementing Measurement-Based Care in Behavioral Health: A Review, doi:10.1001/jamapsychiatry.2018.3329
Miller, S.D., Hubble, M.A., Chow, D., & Seidel, J. (2015). Beyond measures and monitoring: Realizing the potential of feedback-informed treatment. Psychotherapy, 52:4, 449-457.
Pincus, H. and Fleet, A. (2022) “Value Based Payments and Behavioral Health.” JAMA Psychiatry.
Robinsonia, L., Delgadilo, J., & Kellett, S. (2019). The dose-response effect in routinely delivered psychological therapies: A systematic review. Psychotherapy Research, (December 29)
Wampold, B.E. (2015). Routine outcome monitoring: Coming of age—With the usual developmental challenges. Psychotherapy, 52:4, 458-462.
Williams, A.R., et al. (2022). “Performance Measurement for Opioid Use Disorder Medicating Treatment and Care Retention.” American Journal of Psychiatry
Youn, S.J., Kraus, D.R., & Castonguay, L.G. (2012). The treatment outcome package: Facilitating practice and clinically relevant research. Psychotherapy, 49:2, 115-122.
Online References
Risk Matters – It’s all about objectives.
https://www.irisintelligence.com/blog/risk-matters-its-all-about-objectives/#:~:text=This%20explicit%20link%20between%20risk,we%20are%20trying%20to%20achieveBehavioral Health Workforce Report to the Oregon Health Authority and State Legislature FINAL REPORT. https://www.oregon.gov/oha/ERD/SiteAssets/Pages/Government-Relations/Behavioral%20Health%20Workforce%20Wage%20Study%20Report-Final%20020122.pdf
Routine Outcome Monitoring (ROM) and Feedback: Research Review and Recommendations. https://doi.org/10.1080/10503307.2023.2181114
Medicare physician pay cuts underscore need to fix broken system.
https://www.ama-assn.org/practice-management/medicare-medicaid/medicare-physician-pay-cuts-underscore-need-fix-broken-system#:~:text=What's%20the%20news%3A%20U.S.%20physicians,deal%20struck%20by%20congressional%20leadersDefining and Implementing Value-Based Health Care: A Strategic Framework.
https://pubmed.ncbi.nlm.nih.gov/31833857/What is a Contract of Adhesion?
https://ironcladapp.com/journal/contracts/contract-of-adhesion/Most Office-Based Physicians Accept New Patients, Including Patients with Medicare and Private Insurance. https://www.kff.org/medicare/issue-brief/most-office-based-physicians-accept-new-patients-including-patients-with-medicare-and-private-insurance/
The Need for a Measurement-Based Care Professional Practice Guideline.
https://societyforpsychotherapy.org/wp-content/uploads/2023/04/Boswell-et-al-2023.pdf2023 Sustainable Health Care Cost Growth Target Annual Report.
https://www.cms.gov/files/document/nhe-projections-forecast-summary.pdfNational Health Expenditure Projections, 2022–31: Growth To Stabilize Once The COVID-19 Public Health Emergency Ends. https://www.healthaffairs.org/doi/10.1377/hlthaff.2023.00403.
Oregon is the first state in the nation to constitutionally guarantee access to care. Measure 111 passes, giving Oregonians a constitutional right to access affordable health care.
https://www.opb.org/article/2022/11/15/oregon-election-right-to-affordable-health-care/Oregon outpacing national increases in health care costs, study shows.
https://www.opb.org/article/2022/04/27/study-oregon-outpacing-national-increases-in-health-care-costs/"Spike in Telehealth Spending for Mental Health May Drive Payers to Push Back on ‘New Status Quo’". https://tinyl.io/9Gbp
2023 Sustainable Health Care Cost Growth Target Annual Report
https://www.oregon.gov/oha/hpa/hp/pages/sustainable-health-care-cost-growth-target.aspx
Charting a Sustainable Path for Health Care Spending.
https://www.oregon.gov/oha/HPA/HP/HCCGBDocsCost-Growth-Target-Overview.
https://www.oregon.gov/oha/HPA/HP/HCCGBDocs/Cost-Growth-Target-Overview.pdfHealth Care Cost Growth Trends in Oregon, 2020-2021. https://www.oregon.gov/oha/HPA/HP/Cost%20Growth%20Target%20Meeting%20Documents/Oregon-Cost-Growth-Target-Annual-Report%202020-2021.pdf
Frequently Asked Questions about Oregon’s Value-Based Payment Compact.
https://orhealthleadershipcouncil.org/oregon-value-based-payment-compact /https://orhealthleadershipcouncil.org/wp-content/uploads/2021/09/VBP-Compact-FAQ-07.27.21.pdf
The Oregon Value-based Payment Compact represents a collaborative partnership to advance the adoption of value-based payment across the state.
https://www.irmi.com/CY 2024 Medicare Physician Payment Schedule and Quality Payment Program (QPP) Proposed Rule Summary. https://www.ama-assn.org/system/files/ama-summary-2024-mfs-proposed-rule.pdf
What Is Pay for Performance in Healthcare? https://catalyst.nejm.org/doi/full/10.1056/CAT.18.0245
Incentives for Better Performance in Health Care. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC3121024/
Incentive Compensation Practices: A Report on the Horizontal Review of Practices at Large Banking Organizations. https://www.federalreserve.gov/publications/other-reports/incentive-compensation-report-201110.htm
Value-based payment in implementing evidence-based care: the Mental Health Integration Program in Washington State. https://pubmed.ncbi.nlm.nih.gov/28141930/
Designing & Valuing Quality Incentive Programs for Physicians.
https://vmghealth.com/thought-leadership/blog/how-to-structure-a-quality-incentive-program-for-physicians/Can We Pay for Performance in Behavioral Health Care?
https://ps.psychiatryonline.org/doi/10.1176/appi.ps.201600475Why Is Quality Not Improving Quicker?
https://www.healingmagazine.org/pay-for-performance-in-behavioral-healthcare-why-is-quality-not-improving-quicker/Value-Based Payment Technical Guide: Oregon Health Authority.
https://www.oregon.gov/oha/HPA/dsi-tc/Documents/OHA-CCO-VBP-Technical-Guide.pdfValue-based Payment Toolkit for CCOs: Oregon Health Authority.
https://www.oregon.gov/oha/HPA/dsi-tc/Documents/VBP-Contracting-Elements-Brief.pdfAn Analysis of Pay-for-Performance Schemes and Their Potential Impacts on Health Systems and Outcomes for Patients. https://pubmed.ncbi.nlm.nih.gov/31321097/
Large Stakes and Big Mistakes.
https://www.bostonfed.org/publications/research-department-working-paper/2005/large-stakes-and-big-mistakes.aspxPhantom Networks: Discrepancies Between Reported And Realized Mental Health Care Access In Oregon Medicaid. https://www.healthaffairs.org/doi/10.1377/hlthaff.2022.00052
Study: Phantom Providers Rife In Orgon.
https://www.thelundreport.org/content/study-phantom-providers-rife-oregon-health-plan#:~:text=The%20study's%20findings%20include%3A,care%20and%20mental%20health%20providersThe why, what, where, and how of value-based contracts.
https://bulletin.facs.org/2021/06/the-why-what-where-and-how-of-value-based-contracts/Ethical Informed Consent Motivates Patients to Game and Subvert Outcome Measures.
https://www.amha-or.com/informed-consent-motivate-patients-to-game-outcome-measuresWhat is Value-Based Contracting (VBC) for Independent Psychotherapy Practice?
https://www.amha-or.com/value-based-contracting-for-independent-psychotherapy-practiceWhere are all the psychotherapists?
https://www.amha-or.com/where-are-the-psychotherapistsThe Cost and Dangers of Giving Healthplans Your Patients’ Assessment Data.
https://www.amha-or.com/do-not-give-healthplan-your-patients-data-talking-pointsState of Mental Health in America.
https://mhanational.org/sites/default/files/2023-State-of-Mental-Health-in-America-Report.pdf
Statement of Purpose and Background: This article is based on investigation and research regarding requirements for successful implementation of Value Based Reimbursements (VBR), FFS, APM, and VBPs. This article requires study and is not written for lay people seeking a quick read to gain expert awareness. There are many purposes of this paper, the most important of which education and to encourage practice providers to ask questions and learn more about FFS, APM, and VBP contracts where measurement-based care (MBC), pay-for performance (P4P) and outcome informed care (OIC) are the touchpoints for mental and behavioral healthcare contracts design and implementation. This paper also presents for discussion what should not be done with reference to one Healthplan’s proposal. Guidance for this article has been drawn from provider practices, professional associations, thought leaders, industry consultants, the Oregon Health Authority (OHA), the Department of Health and Human Services Health Payment Center Learning Action Network (HPC-LAN), and the Oregon Value-Based Payment Compact (ORCompact). The purpose of this document is to offer readers and decision makers basic understanding of important issues that pertain to FFS, APM and VBP contracting, with a pathway to develop contracts in partnership with Healthplans. Such a pathway will require clear standards for contracting, managed within proposed legislative guidelines which protects the public interest and assures access to mental, behavioral and substance abuse treatment services. This includes commercial contracts, Medicare, Medicaid and employer insurance payers in Oregon and in ways that are not subject to Federal restrictions such a the Federal Trade Commission and Antitrust.
Living Document: This article is a living document that will be revised as new information is made available. The article is for educational and training purposes. Questions and feedback can be submitted by contacting MRI.
Disclaimer: The paper is intended to raise issues that relate to the legal and ethical relationships of mental health practices and healthcare operations support services. This article is a living document that will be revised as new information is made available. The article is for educational discussion and training purposes. Questions and feedback can be submitted by contacting MRI.
The issues discussed in this article are potential conflicts of interests between a type of healthcare operations support business and covered entities who benefit from the services of such businesses. The opinions and concerns expressed do not represent nor should they be taken as legal advice. Any comments posted are not necessarily shared by the authors or the Board of Mentor Research Institute.
Statements, concerns and reasons for those concerns have been presented to encourage discussion among the mental health professionals, legislators, and by regulatory bodies. Healthcare X’s is one example of contracting behavior which some Healthplans are adopting in Oregon. Conclusions about Healthplan X may be revised as new information is available.
Copyright 2024, Mentor Research Institute