Ethical and Legal Requirements for Dating, Matchmaking, Coaching, and Relationship Services
Multidisciplinary Comparison
Mentor Research Institute (2026)
Overview
Dating, matchmaking, coaching, and relationship services operate in unusually intimate areas of a person’s life. Providers and platforms may obtain information concerning loneliness, sexuality, trauma, rejection, family expectations, health, finances, identity, personal preferences, and relationship history. The emotional vulnerability and sensitivity of this information create foreseeable risks of coercion, exploitation, misrepresentation, confidentiality breaches, boundary violations, discrimination, conflicts of interest, and practice beyond competence.
In this practice brief, matchmaking includes two related but distinct activities. First, it may refer to a person who reviews the characteristics, preferences, circumstances, and stated goals of two or more people and uses professional or personal judgment to recommend or arrange an introduction. Second, it may refer to the matching functions and relationship services provided through a dating application, including profile discovery, search tools, compatibility measures, recommendations, eligibility criteria, introductions, communications, screening, and other platform features intended to facilitate contact between members. The ethical responsibilities associated with these activities depend on the provider’s role, qualifications, representations, access to sensitive information, and degree of influence over participant decisions.
This paper applies ethical principles and enforceable standards drawn from the American Psychological Association, American Association for Marriage and Family Therapy, American Counseling Association, and National Association of Social Workers. These professional codes are not interchangeable. They apply to members of their respective professions and may also be incorporated into licensing rules, employment requirements, contracts, certification standards, or standards of care. Licensed professionals remain accountable to their professional responsibilities when they provide psychotherapy, coaching, matchmaking, consultation, education, assessment, or other relationship-related services under their professional identity.
The strongest and generally safest level of professional service is provided by a licensed mental health professional who has also completed relevant specialty education or certification in dating, matchmaking, coaching, and relationship services. Licensure ordinarily establishes governmental verification of education, supervised experience, examination, lawful scope of practice, continuing accountability, and access to a formal complaint and disciplinary process. Relevant specialty certification may add focused preparation concerning dating services, matchmaking practices, screening, informed consent, boundaries, conflicts of interest, privacy, relationship safety, and the distinctions between clinical and nonclinical services. Together, licensure and relevant specialty preparation provide the most complete structure for competence, accountability, consumer protection, and professional recourse. They do not, however, guarantee that a provider will act ethically or that a service will be safe, effective, or successful.
A certified but unlicensed provider may have completed meaningful specialty education and may be accountable to a certifying organization’s standards, complaint procedures, or renewal requirements. Certification can provide evidence of additional preparation, but it does not create a professional license, establish governmental authority to diagnose or treat mental disorders, or provide access to a licensing board’s disciplinary system. The protective value of certification therefore depends on the rigor, independence, transparency, enforcement procedures, and continuing requirements of the certifying organization. Certified but unlicensed providers should accurately describe their qualifications, avoid implying that certification is equivalent to licensure, remain within the lawful limits of coaching or matchmaking, and refer clients for licensed clinical services when assessment or treatment is indicated.
An unlicensed and uncertified provider may offer lawful coaching, matchmaking, educational, or dating-related services, but the public may have no independent verification of the provider’s education, supervised experience, competence, ethical preparation, or accountability. Such providers are not automatically governed by the professional codes reproduced in this paper and may not be subject to either a licensing board or a meaningful certification process. They remain subject to applicable consumer-protection laws, privacy obligations, contracts, advertising requirements, negligence standards, and laws governing the unauthorized practice of licensed professions. The absence of licensure and certification does not establish that a provider is unsafe, but it provides fewer independently verified safeguards and fewer profession-specific avenues for public protection or complaint resolution.
Ethical duties must also be distinguished from legal requirements. Statutes, licensing-board rules, consumer-protection laws, privacy laws, contracts, payer requirements, platform policies, and certification standards may impose additional or different obligations. When an applicable professional code, certification requirement, contractual duty, or law differs from another standard, the provider should identify the controlling requirement, obtain appropriate consultation when the risk or uncertainty is greater than minimal, and comply with the higher standard when required by professional ethics, law, or contract.
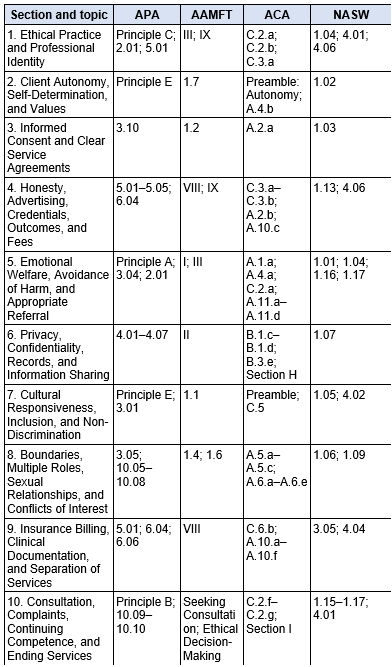
Cross-Professional Standards Map
This table identifies the professional provisions reproduced in full within each section. It is a navigation aid and does not replace the complete quoted source text.
Section 1: Ethical Practice and Professional Identity
Ethical practice begins with a truthful description of who the provider is, what service is being offered, and what professional relationship is being created. A licensed clinician may provide psychotherapy, coaching, education, consultation, or matchmaking-related services, but the label placed on the service does not by itself determine its clinical or legal character. The actual purpose, methods, representations, records, risks, and client expectations matter.
A provider should define in writing whether the service is psychotherapy, nonclinical coaching, matchmaking, or a combined service. The agreement should explain the provider’s credentials, the limits of the service, whether diagnosis or treatment will occur, how emergencies will be handled, and whether insurance will be billed. A clinician should not relabel psychotherapy as coaching to avoid documentation, informed-consent, licensing, or payer requirements. Conversely, nonclinical coaching should not be described in a manner that implies diagnosis, treatment, or a clinical outcome.
Applicable ethical guidance.
APA Principle C and Standards 2.01 and 5.01 require competence and prohibit false or deceptive professional statements. AAMFT Standard III requires professional competence and integrity, and Standard IX governs truthful advertising. ACA Standards C.2.a–C.2.b require practice within competence and appropriate preparation for a new specialty; C.3.a requires accurate advertising. NASW Standards 1.04 and 4.01 limit practice to demonstrated competence, while 4.06 prohibits misrepresentation. Applied here, the provider must use titles, service descriptions, and clinical claims that accurately communicate the provider’s qualifications and the actual nature of the service.
Complete cited source text
American Psychological Association (APA)
Principle C: Integrity
Psychologists seek to promote accuracy, honesty, and truthfulness in the science, teaching, and practice of psychology. In these activities psychologists do not steal, cheat, or engage in fraud, subterfuge, or intentional misrepresentation of fact. Psychologists strive to keep their promises and to avoid unwise or unclear commitments. In situations in which deception may be ethically justifiable to maximize benefits and minimize harm, psychologists have a serious obligation to consider the need for, the possible consequences of, and their responsibility to correct any resulting mistrust or other harmful effects that arise from the use of such techniques.
Standard 2.01: Boundaries of Competence
(a) Psychologists provide services, teach, and conduct research with populations and in areas only within the boundaries of their competence, based on their education, training, supervised experience, consultation, study, or professional experience.
(b) Where scientific or professional knowledge in the discipline of psychology establishes that an understanding of factors associated with age, gender, gender identity, race, ethnicity, culture, national origin, religion, sexual orientation, disability, language, or socioeconomic status is essential for effective implementation of their services or research, psychologists have or obtain the training, experience, consultation, or supervision necessary to ensure the competence of their services, or they make appropriate referrals, except as provided in Standard 2.02, Providing Services in Emergencies.
(c) Psychologists planning to provide services, teach, or conduct research involving populations, areas, techniques, or technologies new to them undertake relevant education, training, supervised experience, consultation, or study.
(d) When psychologists are asked to provide services to individuals for whom appropriate mental health services are not available and for which psychologists have not obtained the competence necessary, psychologists with closely related prior training or experience may provide such services in order to ensure that services are not denied if they make a reasonable effort to obtain the competence required by using relevant research, training, consultation, or study.
(e) In those emerging areas in which generally recognized standards for preparatory training do not yet exist, psychologists nevertheless take reasonable steps to ensure the competence of their work and to protect clients/patients, students, supervisees, research participants, organizational clients, and others from harm.
(f) When assuming forensic roles, psychologists are or become reasonably familiar with the judicial or administrative rules governing their roles.
Standard 5.01: Avoidance of False or Deceptive Statements
(a) Public statements include but are not limited to paid or unpaid advertising, product endorsements, grant applications, licensing applications, other credentialing applications, brochures, printed matter, directory listings, personal resumes or curricula vitae, or comments for use in media such as print or electronic transmission, statements in legal proceedings, lectures and public oral presentations, and published materials. Psychologists do not knowingly make public statements that are false, deceptive, or fraudulent concerning their research, practice, or other work activities or those of persons or organizations with which they are affiliated.
(b) Psychologists do not make false, deceptive, or fraudulent statements concerning (1) their training, experience, or competence; (2) their academic degrees; (3) their credentials; (4) their institutional or association affiliations; (5) their services; (6) the scientific or clinical basis for, or results or degree of success of, their services; (7) their fees; or (8) their publications or research findings.
(c) Psychologists claim degrees as credentials for their health services only if those degrees (1) were earned from a regionally accredited educational institution or (2) were the basis for psychology licensure by the state in which they practice.
American Association for Marriage and Family Therapy (AAMFT)
STANDARD III: PROFESSIONAL COMPETENCE AND INTEGRITY
Marriage and family therapists maintain high standards of professional competence and integrity.
3.1 Maintenance of Competency. Marriage and family therapists pursue knowledge of new developments and emerging therapeutic approaches. Marriage and family therapists maintain their competence in the field through education, training, or supervised experience.
3.2 Knowledge of Regulatory Standards. Marriage and family therapists pursue appropriate education, training, or consultation to ensure adequate knowledge of, and adherence to, applicable laws, ethics, and professional standards.
3.3 Seek Assistance. Marriage and family therapists must not engage in therapeutic services when those services are compromised due to impairments to their clinical competence. Marriage and family therapists seek appropriate supervision, consultation, or professional assistance for issues that may impair work performance or clinical judgment.
3.4 Conflicts of Interest. Marriage and family therapists do not knowingly provide services that create a conflict of interest that may impair work performance, compromise clinical judgment, or cause harm to a client.
3.5 Maintenance of Records. Marriage and family therapists maintain accurate and adequate clinical and financial records in accordance with professional standards and applicable law.
3.6 Development of New Skills. While developing new skills in specialty areas, marriage and family therapists take steps to ensure the competence of their work and to protect clients from possible harm. Marriage and family therapists practice in specialty areas new to them only after appropriate education, training, or supervised experience.
3.7 Harassment. Marriage and family therapists must not engage in sexual or other forms of harassment of clients, students, trainees, supervisees, employees, colleagues, research participants, or other persons with whom they have a professional relationship.
3.8 Exploitation. Recognizing the potential for power imbalances, marriage and family therapists do not exploit clients, students, trainees, supervisees, employees, colleagues, research participants, or other persons with whom they have a professional relationship.
3.9 Gifts. When deciding whether or not to accept from or give gifts to clients, marriage and family therapists consider cultural norms and meaning, professional standards, and client perceptions. Marriage and family therapists consider the potential effects that receiving or giving gifts may have on clients and the therapeutic relationship.
3.10 Scope of Competence. Marriage and family therapists do not diagnose, treat, or advise on problems outside the recognized boundaries of their competencies.
3.11 Public Statements. Marriage and family therapists, because of their ability to influence and alter the lives of others and the public perception of the profession, adhere to professional standards when making professional recommendations or giving opinions through testimony or other public statements.
3.12 Professional Misconduct. Marriage and family therapists may be in violation of this Code and subject to termination of membership or other appropriate action if they: (a) are convicted of any felony; (b) are convicted of a misdemeanor related to their qualifications or functions; (c) engage in conduct which could lead to conviction of a felony, or a misdemeanor related to their qualifications or functions; (d) are expelled from or disciplined by other professional organizations; (e) have their licenses or certificates suspended or revoked, or are subject to any order, settlement, or disciplinary action by a regulatory body; (f) continue to practice marriage and family therapy while no longer competent to do so because they are impaired by physical or mental causes or the abuse of alcohol or other substances; or (g) fail to cooperate with the Association at any point from the inception of an ethical complaint through the completion of all proceedings regarding that complaint.
STANDARD IX: ADVERTISING
Marriage and family therapists only engage in appropriate networking, advertising, and marketing activities.
9.1 Accurate Professional Representation. Marriage and family therapists accurately represent their affiliations, licensure, supervision status, educational degrees, competencies, training, and experience associated with the practice of marriage and family therapy, complying with applicable law.
9.2 Promotional Materials. Marriage and family therapists ensure that advertisements and publications in any and all media are true, accurate, and comply with applicable law and professional standards. Marriage and family therapists do not solicit testimonials or endorsements from current clients or from other persons who are vulnerable to undue influence.
9.3 Educational Credentials. Marriage and family therapists do not advertise or claim educational degrees for clinical services that do not demonstrate training and education in marriage and family therapy or related fields.
9.4 Employee, Contractor, or Supervisee Qualifications. Marriage and family therapists reasonably ensure that the qualifications of their employees, contractors, and supervisees are represented in a manner that is true, accurate, and in accordance with applicable law.
9.5 Specialization. Marriage and family therapists represent themselves as providing specialized services only after taking reasonable steps to ensure the competence of their work and to protect clients, supervisees, and others from harm.
9.6 Correction of Misinformation. Marriage and family therapists make reasonable efforts to correct false, misleading, or inaccurate information and representations made on their behalf by others concerning the therapist’s qualifications, services, or products.
American Counseling Association (ACA)
ACA Standard C.2.a: Boundaries of Competence
Counselors practice only within the boundaries of their competence, based on their education, training, supervised experience, state and national professional credentials, and appropriate professional experience. Whereas multicultural counseling competency is required across all counseling specialties, counselors gain knowledge, personal awareness, sensitivity, dispositions, and skills pertinent to being a culturally competent counselor in working with a diverse client population.
ACA Standard C.2.b: New Specialty Areas of Practice
Counselors practice in specialty areas new to them only after appropriate education, training, and supervised experience. While developing skills in new specialty areas, counselors take steps to ensure the competence of their work and protect others from possible harm.
ACA Standard C.3.a: Accurate Advertising
When advertising or otherwise representing their services to the public, counselors identify their credentials in an accurate manner that is not false, misleading, deceptive, or fraudulent.
National Association of Social Workers (NASW)
NASW Standard 1.04: Competence
(a) Social workers should provide services and represent themselves as competent only within the boundaries of their education, training, license, certification, consultation received, supervised experience, or other relevant professional experience.
(b) Social workers should provide services in substantive areas or use intervention techniques or approaches that are new to them only after engaging in appropriate study, training, consultation, and supervision from people who are competent in those interventions or techniques.
(c) When generally recognized standards do not exist with respect to an emerging area of practice, social workers should exercise careful judgment and take responsible steps (including appropriate education, research, training, consultation, and supervision) to ensure the competence of their work and to protect clients from harm.
(d) Social workers who use technology in the provision of social work services should ensure that they have the necessary knowledge and skills to provide such services in a competent manner. This includes an understanding of the special communication challenges when using technology and the ability to implement strategies to address these challenges.
(e) Social workers who use technology in providing social work services should comply with the laws governing technology and social work practice in the jurisdiction in which they are regulated and located and, as applicable, in the jurisdiction in which the client is located.
NASW Standard 4.01: Competence
(a) Social workers should accept responsibility or employment only on the basis of existing competence or the intention to acquire the necessary competence.
(b) Social workers should strive to become and remain proficient in professional practice and the performance of professional functions. Social workers should critically examine and keep current with emerging knowledge relevant to social work. Social workers should
routinely review the professional literature and participate in continuing education relevant to social work practice and social work ethics.
(c) Social workers should base practice on recognized knowledge, including empirically based knowledge, relevant to social work and social work ethics.
NASW Standard 4.06: Misrepresentation
(a) Social workers should make clear distinctions between statements made and actions engaged in as a private individual and as a representative of the social work profession, a professional social work organization, or the social worker’s employing agency.
(b) Social workers who speak on behalf of professional social work organizations should accurately represent the official and authorized positions of these organizations.
(c) Social workers should ensure that their representations to clients, agencies, and the public of professional qualifications, credentials, education, competence, affiliations, services provided, or results to be achieved are accurate. Social workers should claim only those relevant professional credentials they actually possess and take steps to correct any inaccuracies or misrepresentations of their credentials by others.
Section 2: Client Autonomy, Self-Determination, and Values
Clients retain authority over whether to date, whom to date, what characteristics matter to them, whether to continue a relationship, and whether to accept a provider’s recommendation. The provider may offer observations, challenge internal inconsistencies, explain foreseeable consequences, and help clients examine preferences. The provider should not pressure a client to accept a match, alter a core value, disclose information, purchase additional services, or continue dating when the client wishes to pause.
Autonomy does not require passive agreement with every client preference. A provider may respectfully identify bias, unrealistic expectations, safety concerns, or contradictions between stated goals and behavior. The ethical distinction is between assisting reflection and imposing the provider’s own moral, religious, political, cultural, or relational values. Advice should be offered transparently, with the client’s right to decline preserved.
Applicable ethical guidance.
APA Principle E protects dignity, privacy, and self-determination. AAMFT Standard 1.7 requires respect for client autonomy in decision-making. ACA identifies autonomy as a foundational principle and Standard A.4.b directs counselors to avoid imposing their own values. NASW Standard 1.02 states that social workers respect and promote clients’ right to self-determination and help clients clarify their goals, subject to limited safety exceptions. Therefore, a provider may educate, question, and recommend, but should not coerce a relational decision or substitute the provider’s values for the client’s.
Complete cited source text
American Psychological Association (APA)
Principle E: Respect for People’s Rights and Dignity
Psychologists respect the dignity and worth of all people, and the rights of individuals to privacy, confidentiality, and self-determination. Psychologists are aware that special safeguards may be necessary to protect the rights and welfare of persons or communities whose vulnerabilities impair autonomous decision making. Psychologists are aware of and respect cultural, individual, and role differences, including those based on age, gender, gender identity, race, ethnicity, culture, national origin, religion, sexual orientation, disability, language, and socioeconomic status, and consider these factors when working with members of such groups. Psychologists try to eliminate the effect on their work of biases based on those factors, and they do not knowingly participate in or condone activities of others based upon such prejudices.
American Association for Marriage and Family Therapy (AAMFT)
AAMFT Standard 1.7
1.7 Client Autonomy in Decision Making. Marriage and family therapists must respect the rights of clients to make decisions and help them to understand the consequences of these decisions. Marriage and family therapists clearly advise clients that clients have the responsibility to make decisions regarding relationships such as cohabitation, marriage, divorce, separation, reconciliation, custody, and visitation or parenting time.
American Counseling Association (ACA)
ACA Code of Ethics Preamble — Autonomy or fostering the right to control the direction of one’s life;
ACA Standard A.4.b: Personal Values
Counselors are aware of—and avoid imposing—their own values, attitudes, beliefs, and behaviors. Counselors respect the diversity of clients, trainees, and research participants and seek training in areas in which they are at risk of imposing their values onto clients, especially when the counselor’s values are inconsistent with the client’s goals or are discriminatory in nature.
National Association of Social Workers (NASW)
NASW Standard 1.02: Self-Determination
Social workers respect and promote the right of clients to self-determination and assist clients in their efforts to identify and clarify their goals. Social workers may limit clients’ right to self-determination when, in the social workers’ professional judgment, clients’ actions or potential actions pose a serious, foreseeable, and imminent risk to themselves or others.
Section 3: Informed Consent and Clear Service Agreements
Informed consent is an ongoing process, not merely a signature obtained at intake. Before services begin, clients should receive understandable information about the purpose and methods of the service; provider credentials; anticipated benefits and material risks; alternatives; fees and refunds; privacy practices; electronic communication; recordkeeping; complaint procedures; termination; and the limits of confidentiality. Clients should have an opportunity to ask questions and should be informed of material changes as services evolve.
When one provider offers both psychotherapy and coaching, the client should understand which role applies at a given time, whether separate agreements and records are used, and how transitions will be managed. A disclaimer that coaching is not therapy is insufficient when the provider is actually assessing, diagnosing, or treating a mental disorder. Likewise, consent should identify whether information may be shared with a dating platform, matchmaker, referring professional, partner, family member, or other third party.
Applicable ethical guidance. APA Standard 3.10 requires informed consent using reasonably understandable language. AAMFT requires appropriate informed consent before therapy or related procedures and as needed throughout services. ACA Standard A.2.a requires clients to receive adequate information about counseling and the right to participate in the plan. NASW Standard 1.03 specifically requires clear information about purpose, risks, limitations, costs, alternatives, refusal or withdrawal, and the period covered by consent. The practical requirement is a service-specific, understandable agreement that accurately describes what will occur and is revisited when the role or service changes.
Complete cited source text
American Psychological Association (APA)
Standard 3.10: Informed Consent
(a) When psychologists conduct research or provide assessment, therapy, counseling, or consulting services in person or via electronic transmission or other forms of communication, they obtain the informed consent of the individual or individuals using language that is reasonably understandable to that person or persons except when conducting such activities without consent is mandated by law or governmental regulation or as otherwise provided in this Ethics Code. (See also Standards 8.02, Informed Consent to Research; 9.03, Informed Consent in Assessments; and 10.01, Informed Consent to Therapy.)
(b) For persons who are legally incapable of giving informed consent, psychologists nevertheless (1) provide an appropriate explanation, (2) seek the individual’s assent, (3) consider such persons’ preferences and best interests, and (4) obtain appropriate permission from a legally authorized person, if such substitute consent is permitted or required by law. When consent by a legally authorized person is not permitted or required by law, psychologists take reasonable steps to protect the individual’s rights and welfare.
(c) When psychological services are court ordered or otherwise mandated, psychologists inform the individual of the nature of the anticipated services, including whether the services are court ordered or mandated and any limits of confidentiality, before proceeding.
(d) Psychologists appropriately document written or oral consent, permission, and assent. (See also Standards 8.02, Informed Consent to Research; 9.03, Informed Consent in Assessments; and 10.01, Informed Consent to Therapy.)
American Association for Marriage and Family Therapy (AAMFT)
AAMFT Standard 1.2
1.2 Informed Consent. Prior to initiating services, and as often as necessary throughout treatment, marriage and family therapists obtain appropriate informed consent to therapy or related procedures and use language that is reasonably understandable to clients. When persons, due to age or mental status, are legally incapable of giving informed consent, marriage and family therapists obtain informed permission from a legally authorized person, as permitted by law. The content of informed consent may vary depending upon the client and treatment plan; however, informed consent generally necessitates that the client: (a) has the capacity to consent; (b) has been adequately informed of significant information concerning treatment processes and procedures; (c) has been adequately informed of potential risks and benefits of treatments; (d) has freely and without undue influence expressed consent; and (e) has provided consent that is appropriately documented.
American Counseling Association (ACA)
ACA Standard A.2.a: Informed Consent
Clients have the freedom to choose whether to enter into or remain in a counseling relationship and need adequate information about the counseling process and the counselor. Counselors have an obligation to review in writing and verbally with clients the rights and responsibilities of both counselors and clients. Informed consent is an ongoing part of the counseling process, and counselors appropriately document discussions of informed consent throughout the counseling relationship.
National Association of Social Workers (NASW)
NASW Standard 1.03: Informed Consent
(a) Social workers should provide services to clients only in the context of a professional relationship based, when appropriate, on valid informed consent. Social workers should use clear and understandable language to inform clients of the purpose of the services, risks related to the services, limits to services because of the requirements of a third-party payer, relevant costs, reasonable alternatives, clients’ right to refuse or withdraw consent, and the time frame covered by the consent. Social workers should provide clients with an opportunity to ask questions.
(b) In instances when clients are not literate or have difficulty understanding the primary language used in the practice setting, social workers should take steps to ensure clients’ comprehension. This may include providing clients with a detailed verbal explanation or arranging for a qualified interpreter or translator whenever possible.
(c) In instances when clients lack the capacity to provide informed consent, social workers should protect clients’ interests by seeking permission from an appropriate third party, informing clients consistent with their level of understanding. In such instances social workers should seek to ensure that the third party acts in a manner consistent with clients’ wishes and interests. Social workers should take reasonable steps to enhance such clients’ ability to give informed consent.
(d) In instances when clients are receiving services involuntarily, social workers should provide information about the nature and extent of services and about the extent of clients’ right to refuse service.
(e) Social workers should discuss with clients the social workers’ policies concerning the use of technology in the provision of professional services.
(f) Social workers who use technology to provide social work services should obtain informed consent from the individuals using these services during the initial screening or interview and prior to initiating services. Social workers should assess clients’ capacity to provide informed consent and, when using technology to communicate, verify the identity and location of clients.
(g) Social workers who use technology to provide social work services should assess the clients’ suitability and capacity for electronic and remote services. Social workers should consider the clients’ intellectual, emotional, and physical ability to use technology to receive services and ability to understand the potential benefits, risks, and limitations of such services. If clients do not wish to use services provided through technology, social workers should help them identify alternate methods of service.
(h) Social workers should obtain clients’ informed consent before making audio or video recordings of clients or permitting observation of service provision by a third party.
(i) Social workers should obtain client consent before conducting an electronic search on the client. Exceptions may arise when the search is for purposes of protecting the client or others from serious, foreseeable, and imminent harm, or for other compelling professional reasons.
Section 4: Honesty, Advertising, Credentials, Outcomes, and Fees
Advertising should describe the process and support offered rather than promise a result that no provider can control. Claims such as “guaranteed soulmate,” “100 percent success,” or “married within 90 days” are ethically problematic unless they are objectively defined, verifiable, appropriately qualified, and not misleading. Testimonials should be genuine, voluntary, and used only with valid authorization. Providers should be especially cautious about requesting testimonials from current psychotherapy clients because the power differential can compromise voluntariness.
Credentials, certifications, experience, success rates, referral relationships, and affiliations must be stated accurately. A provider should not imply licensure, specialty competence, research validation, or endorsement that does not exist. Fees, subscriptions, cancellation terms, refund limitations, package contents, and the number or meaning of introductions should be disclosed before purchase. Scarcity tactics, emotional pressure, and undisclosed automatic renewals can exploit loneliness and urgency.
Applicable ethical guidance.
APA Standards 5.01–5.05 address false statements, advertising, and testimonials, and Standard 6.04 requires fee agreements to be reached as early as feasible. AAMFT Standards VIII and IX govern financial arrangements and advertising. ACA Standards C.3.a–C.3.b require accurate advertising and caution against soliciting testimonials from vulnerable clients; A.2.b requires disclosure of fees and billing arrangements during informed consent, and A.10.c governs establishing fees. NASW Standards 1.13 and 4.06 require fair, reasonable fees and prohibit misrepresentation. These standards require verifiable claims, accurate credentials, noncoercive marketing, and written financial terms provided before the client commits.
Complete cited source text
American Psychological Association (APA)
Standard 5.01: Avoidance of False or Deceptive Statements
(a) Public statements include but are not limited to paid or unpaid advertising, product endorsements, grant applications, licensing applications, other credentialing applications, brochures, printed matter, directory listings, personal resumes or curricula vitae, or comments for use in media such as print or electronic transmission, statements in legal proceedings, lectures and public oral presentations, and published materials. Psychologists do not knowingly make public statements that are false, deceptive, or fraudulent concerning their research, practice, or other work activities or those of persons or organizations with which they are affiliated.
(b) Psychologists do not make false, deceptive, or fraudulent statements concerning (1) their training, experience, or competence; (2) their academic degrees; (3) their credentials; (4) their institutional or association affiliations; (5) their services; (6) the scientific or clinical basis for, or results or degree of success of, their services; (7) their fees; or (8) their publications or research findings.
(c) Psychologists claim degrees as credentials for their health services only if those degrees (1) were earned from a regionally accredited educational institution or (2) were the basis for psychology licensure by the state in which they practice.
Standard 5.02: Statements by Others
(a) Psychologists who engage others to create or place public statements that promote their professional practice, products, or activities retain professional responsibility for such statements.
(b) Psychologists do not compensate employees of press, radio, television, or other communication media in return for publicity in a news item. (See also Standard 1.01, Misuse of Psychologists’ Work.)
(c) A paid advertisement relating to psychologists’ activities must be identified or clearly recognizable as such.
Standard 5.03: Descriptions of Workshops and Non-Degree-Granting Educational Programs
To the degree to which they exercise control, psychologists responsible for announcements, catalogs, brochures, or advertisements describing workshops, seminars, or other non-degree-granting educational programs ensure that they accurately describe the audience for which the program is intended, the educational objectives, the presenters, and the fees involved.
Standard 5.04: Media Presentations
When psychologists provide public advice or comment via print, Internet, or other electronic transmission, they take precautions to ensure that statements (1) are based on their professional knowledge, training, or experience in accord with appropriate psychological literature and practice; (2) are otherwise consistent with this Ethics Code; and (3) do not indicate that a professional relationship has been established with the recipient. (See also Standard 2.04, Bases for Scientific and Professional Judgments.)
Standard 5.05: Testimonials
Psychologists do not solicit testimonials from current therapy clients/patients or other persons who because of their particular circumstances are vulnerable to undue influence.
Standard 6.04: Fees and Financial Arrangements
(a) As early as is feasible in a professional or scientific relationship, psychologists and recipients of psychological services reach an agreement specifying compensation and billing arrangements.
(b) Psychologists’ fee practices are consistent with law.
(c) Psychologists do not misrepresent their fees.
(d) If limitations to services can be anticipated because of limitations in financing, this is discussed with the recipient of services as early as is feasible. (See also Standards 10.09, Interruption of Therapy, and 10.10, Terminating Therapy.)
(e) If the recipient of services does not pay for services as agreed, and if psychologists intend to use collection agencies or legal measures to collect the fees, psychologists first inform the person that such measures will be taken and provide that person an opportunity to make prompt payment. (See also Standards 4.05, Disclosures; 6.03, Withholding Records for Nonpayment; and 10.01, Informed Consent to Therapy.)
American Association for Marriage and Family Therapy (AAMFT)
Standard VIII: Financial Arrangements
STANDARD VIII: FINANCIAL ARRANGEMENTS
Marriage and family therapists make financial arrangements with clients, third-party payors, and supervisees that are reasonably understandable and conform to accepted professional practices and applicable laws.
8.1 Financial Integrity. Marriage and family therapists do not offer or accept kickbacks, rebates, bonuses, or other remuneration for referrals.
8.2 Disclosure of Financial Policies. Prior to entering into the therapeutic or supervisory relationship, marriage and family therapists clearly disclose and explain to clients and supervisees in writing: (a) all financial arrangements and fees related to professional services, including charges for canceled or missed appointments; (b) the use of collection agencies or legal measures for nonpayment; and (c) the policy of obtaining payment from the client, to the extent allowed by law, if payment is denied by the third-party payor. Once services have begun, therapists provide reasonable notice of any changes in fees or other charges.
8.3 Notice of Payment Recovery Procedures. Marriage and family therapists give reasonable notice to clients with unpaid balances of their intent to seek collection by agency or legal recourse. When such action is taken, marriage and family therapists will not disclose clinical information unless permitted or mandated by law.
8.4 Truthful Representation of Services. Marriage and family therapists represent facts truthfully to clients, third-party payors, and supervisees regarding services rendered.
8.5 Bartering. Marriage and family therapists ordinarily refrain from accepting goods and services from clients in return for services rendered. Bartering for professional services may be conducted only if: (a) the supervisee or client requests it; (b) the relationship is not exploitative; (c) the professional relationship is not distorted; (d) a clear written contract is established; and (e) the marriage and family therapist documents the rationale for entering into the bartering agreement.
8.6 Withholding Records for Non-Payment. Marriage and family therapists may not withhold records under their immediate control solely because payment has not been received for past services.
Standard IX: Advertising
STANDARD IX: ADVERTISING Marriage and family therapists only engage in appropriate networking, advertising, and marketing activities.
9.1 Accurate Professional Representation. Marriage and family therapists accurately represent their affiliations, licensure, supervision status, educational degrees, competencies, training, and experience associated with the practice of marriage and family therapy, complying with applicable law.
9.2 Promotional Materials. Marriage and family therapists ensure that advertisements and publications in any and all media are true, accurate, and comply with applicable law and professional standards. Marriage and family therapists do not solicit testimonials or endorsements from current clients or from other persons who are vulnerable to undue influence.
9.3 Educational Credentials. Marriage and family therapists do not advertise or claim educational degrees for clinical services that do not demonstrate training and education in marriage and family therapy or related fields.
9.4 Employee, Contractor, or Supervisee Qualifications. Marriage and family therapists reasonably ensure that the qualifications of their employees, contractors, and supervisees are represented in a manner that is true, accurate, and in accordance with applicable law.
9.5 Specialization. Marriage and family therapists represent themselves as providing specialized services only after taking reasonable steps to ensure the competence of their work and to protect clients, supervisees, and others from harm.
9.6 Correction of Misinformation. Marriage and family therapists make reasonable efforts to correct false, misleading, or inaccurate information and representations made on their behalf by others concerning the therapist’s qualifications, services, or products.
American Counseling Association (ACA)
ACA Standard C.3.a: Accurate Advertising
When advertising or otherwise representing their services to the public, counselors identify their credentials in an accurate manner that is not false, misleading, deceptive, or fraudulent.
ACA Standard C.3.b: Testimonials
Counselors who use testimonials do not solicit them from current clients, former clients, or any other persons who may be vulnerable to undue influence. Counselors discuss with clients the implications of and obtain permission for the use of any testimonial.
ACA Standard A.2.b: Types of Information Needed
Counselors explicitly explain to clients the nature of all services provided. They inform clients about issues such as, but not limited to, the following: the purposes, goals, techniques, procedures, limitations, potential risks, and benefits of services; the counselor’s qualifications, credentials, relevant experience, and approach to counseling; continuation of services upon the incapacitation or death of the counselor; the role of technology; and other pertinent information. Counselors take steps to ensure that clients understand the implications of diagnosis and the intended use of tests and reports. Additionally, counselors inform clients about fees and billing arrangements, including procedures for nonpayment of fees. Clients have the right to confidentiality and to be provided with an explanation of its limits (including how supervisors and/or treatment or interdisciplinary team professionals are involved), to obtain clear information about their records, to participate in the ongoing counseling plans, and to refuse any services or modality changes and to be advised of the consequences of such refusal.
ACA Standard A.10.c: Establishing Fees
In establishing fees for professional counseling services, counselors consider the financial status of clients and locality. If a counselor’s usual fees create undue hardship for the client, the counselor may adjust fees, when legally permissible, or assist the client in locating comparable, affordable services.
National Association of Social Workers (NASW)
NASW Standard 1.13: Payment for Services
(a) When setting fees, social workers should ensure that the fees are fair, reasonable, and commensurate with the services performed. Consideration should be given to clients’ ability to pay.
(b) Social workers should avoid accepting goods or services from clients as payment for professional services. Bartering arrangements, particularly involving services, create the potential for conflicts of interest, exploitation, and inappropriate boundaries in social workers’ relationships with clients. Social workers should explore and may participate in bartering only in very limited circumstances when it can be demonstrated that such arrangements are an accepted practice among professionals in the local community, considered to be essential for the provision of services, negotiated without coercion, and entered into at the client’s initiative and with the client’s informed consent. Social workers who accept goods or services from clients as payment for professional services assume the full burden of demonstrating that this arrangement will not be detrimental to the client or the professional relationship.
(c) Social workers should not solicit a private fee or other remuneration for providing services to clients who are entitled to such available services through the social workers’ employer or agency.
NASW Standard 4.06: Misrepresentation
(a) Social workers should make clear distinctions between statements made and actions engaged in as a private individual and as a representative of the social work profession, a professional social work organization, or the social worker’s employing agency.
(b) Social workers who speak on behalf of professional social work organizations should accurately represent the official and authorized positions of these organizations.
(c) Social workers should ensure that their representations to clients, agencies, and the public of professional qualifications, credentials, education, competence, affiliations, services provided, or results to be achieved are accurate. Social workers should claim only those relevant professional credentials they actually possess and take steps to correct any inaccuracies or misrepresentations of their credentials by others.
Section 5: Emotional Welfare, Avoidance of Harm, and Appropriate Referral
Relationship services should be paced according to the client’s readiness and welfare, not the provider’s sales targets or activity metrics. Repeated rejection, trauma reminders, compulsive app use, stalking, intimate partner violence, suicidality, substance misuse, mania, severe depression, or marked functional impairment may require clinical assessment or specialized care. A coach should not attempt to treat these conditions without the necessary license and competence.
Support should combine hope with realism. Providers should validate distress without making unsupported clinical claims or offering false reassurance. When services are ineffective, contraindicated, or outside scope, the provider should discuss referral, coordination, pausing, or termination. Referral should not be punitive, discriminatory, or used to avoid clients merely because their values differ from the provider’s.
Applicable ethical guidance.
APA Principle A and Standard 3.04 require reasonable steps to avoid harm; Standard 2.01 limits practice to competence. AAMFT Standards I and III prioritize client welfare and competent practice. ACA Standards A.1.a and A.4.a place client welfare first and require avoidance of harm; C.2.a limits practice to competence; A.11 addresses appropriate referral and termination. NASW Standards 1.01, 1.04, 1.16, and 1.17 require commitment to client well-being, competent practice, referral when specialized expertise is needed, and responsible termination. The provider should recognize risk, avoid practicing beyond competence, and arrange appropriate care rather than continuing a service that is not benefiting the client.
Complete cited source text
American Psychological Association (APA)
Principle A: Beneficence and Nonmaleficence
Psychologists strive to benefit those with whom they work and take care to do no harm. In their professional actions, psychologists seek to safeguard the welfare and rights of those with whom they interact professionally and other affected persons, and the welfare of animal subjects of research. When conflicts occur among psychologists’ obligations or concerns, they attempt to resolve these conflicts in a responsible fashion that avoids or minimizes harm. Because psychologists’ scientific and professional judgments and actions may affect the lives of others, they are alert to and guard against personal, financial, social, organizational, or political factors that might lead to misuse of their influence. Psychologists strive to be aware of the possible effect of their own physical and mental health on their ability to help those with whom they work.
Standard 3.04: Avoiding Harm
(a) Psychologists take reasonable steps to avoid harming their clients/patients, students, supervisees, research participants, organizational clients, and others with whom they work, and to minimize harm where it is foreseeable and unavoidable.
(b) Psychologists do not participate in, facilitate, assist, or otherwise engage in torture, defined as any act by which severe pain or suffering, whether physical or mental, is intentionally inflicted on a person, or in any other cruel, inhuman, or degrading behavior that violates 3.04a.
Standard 2.01: Boundaries of Competence
(a) Psychologists provide services, teach, and conduct research with populations and in areas only within the boundaries of their competence, based on their education, training, supervised experience, consultation, study, or professional experience.
(b) Where scientific or professional knowledge in the discipline of psychology establishes that an understanding of factors associated with age, gender, gender identity, race, ethnicity, culture, national origin, religion, sexual orientation, disability, language, or socioeconomic status is essential for effective implementation of their services or research, psychologists have or obtain the training, experience, consultation, or supervision necessary to ensure the competence of their services, or they make appropriate referrals, except as provided in Standard 2.02, Providing Services in Emergencies.
(c) Psychologists planning to provide services, teach, or conduct research involving populations, areas, techniques, or technologies new to them undertake relevant education, training, supervised experience, consultation, or study.
(d) When psychologists are asked to provide services to individuals for whom appropriate mental health services are not available and for which psychologists have not obtained the competence necessary, psychologists with closely related prior training or experience may provide such services in order to ensure that services are not denied if they make a reasonable effort to obtain the competence required by using relevant research, training, consultation, or study.
(e) In those emerging areas in which generally recognized standards for preparatory training do not yet exist, psychologists nevertheless take reasonable steps to ensure the competence of their work and to protect clients/patients, students, supervisees, research participants, organizational clients, and others from harm.
(f) When assuming forensic roles, psychologists are or become reasonably familiar with the judicial or administrative rules governing their roles.
American Association for Marriage and Family Therapy (AAMFT)
Standard I: Responsibility To Clients
STANDARD I: RESPONSIBILITY TO CLIENTS Marriage and family therapists advance the well-being of families, partners, and individuals and make reasonable efforts to find the appropriate balance between conflicting goals within family systems.
1.1 Non-Discrimination. Marriage and family therapists provide professional assistance to persons without discrimination on the basis of race/ethnicity, color, religion, national origin, location, citizenship status, sex (including pregnancy, childbirth, and related medical conditions), sexual orientation, sexual or gender expression, gender identity, disability (physical or mental), age, genetic information, marital status, veteran or military status, or any other characteristic protected by applicable law.
1.2 Informed Consent. Prior to initiating services, and as often as necessary throughout treatment, marriage and family therapists obtain appropriate informed consent to therapy or related procedures and use language that is reasonably understandable to clients. When persons, due to age or mental status, are legally incapable of giving informed consent, marriage and family therapists obtain informed permission from a legally authorized person, as permitted by law. The content of informed consent may vary depending upon the client and treatment plan; however, informed consent generally necessitates that the client: (a) has the capacity to consent; (b) has been adequately informed of significant information concerning treatment processes and procedures; (c) has been adequately informed of potential risks and benefits of treatments; (d) has freely and without undue influence expressed consent; and (e) has provided consent that is appropriately documented.
1.3 Multiple Relationships. Marriage and family therapists must not exploit clients. Marriage and family therapists, therefore, make every effort to avoid multiple relationships or conditions with clients that could impair professional judgment or increase the risk of exploitation. Such relationships include, but are not limited to, business or close personal relationships with a client or the client’s family. When the risk of impairment or exploitation exists due to multiple roles or conditions, marriage and family therapists document the precautions taken.
1.4 Sexual Behavior with Current Clients, Former Clients, and Others. All forms of sexual behavior with current and former clients or with known members of the client’s family system are prohibited.
1.5 Reports of Unethical Behavior. Marriage and family therapists must comply with applicable laws regarding the reporting of alleged unethical conduct.
1.6 Abuse of the Therapeutic Relationship. Marriage and family therapists do not abuse their power in therapeutic relationships.
1.7 Client Autonomy in Decision Making. Marriage and family therapists must respect the rights of clients to make decisions and help them to understand the consequences of these decisions. Marriage and family therapists clearly advise clients that clients have the responsibility to make decisions regarding relationships such as cohabitation, marriage, divorce, separation, reconciliation, custody, and visitation or parenting time.
1.8 Relationship Beneficial to Client. Marriage and family therapists continue therapeutic relationships only as long as it is reasonably clear that clients are benefiting from the relationship.
1.9 Referrals. Marriage and family therapists make reasonable efforts to provide current, former, or prospective clients with appropriate referrals if the marriage and family therapist is unable or unwilling to provide professional help.
1.10 Non-abandonment. Marriage and family therapists do not terminate treatment with clients without making reasonable efforts to provide appropriate arrangements for the continuation of care.
1.11 Written Consent to Record. Marriage and family therapists must obtain informed consent and written authorization from clients or legally authorized persons before recording any images, video, audio, using any transcription services, or permitting third-party observation.
1.12 Relationships with Third Parties. Marriage and family therapists, upon agreeing to provide services to a person or entity at the request of a third party, clarify, to the extent feasible and at the outset of the service, the nature of the relationship with each party and the limits of confidentiality.
Standard III: Professional Competence And Integrity
STANDARD III: PROFESSIONAL COMPETENCE AND INTEGRITY Marriage and family therapists maintain high standards of professional competence and integrity.
3.1 Maintenance of Competency. Marriage and family therapists pursue knowledge of new developments and emerging therapeutic approaches. Marriage and family therapists maintain their competence in the field through education, training, or supervised experience.
3.2 Knowledge of Regulatory Standards. Marriage and family therapists pursue appropriate education, training, or consultation to ensure adequate knowledge of, and adherence to, applicable laws, ethics, and professional standards.
3.3 Seek Assistance. Marriage and family therapists must not engage in therapeutic services when those services are compromised due to impairments to their clinical competence. Marriage and family therapists seek appropriate supervision, consultation, or professional assistance for issues that may impair work performance or clinical judgment.
3.4 Conflicts of Interest. Marriage and family therapists do not knowingly provide services that create a conflict of interest that may impair work performance, compromise clinical judgment, or cause harm to a client.
3.5 Maintenance of Records. Marriage and family therapists maintain accurate and adequate clinical and financial records in accordance with professional standards and applicable law.
3.6 Development of New Skills. While developing new skills in specialty areas, marriage and family therapists take steps to ensure the competence of their work and to protect clients from possible harm. Marriage and family therapists practice in specialty areas new to them only after appropriate education, training, or supervised experience.
3.7 Harassment. Marriage and family therapists must not engage in sexual or other forms of harassment of clients, students, trainees, supervisees, employees, colleagues, research participants, or other persons with whom they have a professional relationship.
3.8 Exploitation. Recognizing the potential for power imbalances, marriage and family therapists do not exploit clients, students, trainees, supervisees, employees, colleagues, research participants, or other persons with whom they have a professional relationship.
3.9 Gifts. When deciding whether or not to accept from or give gifts to clients, marriage and family therapists consider cultural norms and meaning, professional standards, and client perceptions. Marriage and family therapists consider the potential effects that receiving or giving gifts may have on clients and the therapeutic relationship.
3.10 Scope of Competence. Marriage and family therapists do not diagnose, treat, or advise on problems outside the recognized boundaries of their competencies.
3.11 Public Statements. Marriage and family therapists, because of their ability to influence and alter the lives of others and the public perception of the profession, adhere to professional standards when making professional recommendations or giving opinions through testimony or other public statements.
3.12 Professional Misconduct. Marriage and family therapists may be in violation of this Code and subject to termination of membership or other appropriate action if they: (a) are convicted of any felony; (b) are convicted of a misdemeanor related to their qualifications or functions; (c) engage in conduct which could lead to conviction of a felony, or a misdemeanor related to their qualifications or functions; (d) are expelled from or disciplined by other professional organizations; (e) have their licenses or certificates suspended or revoked, or are subject to any order, settlement, or disciplinary action by a regulatory body; (f) continue to practice marriage and family therapy while no longer competent to do so because they are impaired by physical or mental causes or the abuse of alcohol or other substances; or (g) fail to cooperate with the Association at any point from the inception of an ethical complaint through the completion of all proceedings regarding that complaint.
American Counseling Association (ACA)
ACA Standard A.1.a: Primary Responsibility
The primary responsibility of counselors is to respect the dignity and promote the welfare of clients.
ACA Standard A.4.a: Avoiding Harm
Counselors act to avoid harming their clients, trainees, and research participants and to minimize or to remedy unavoidable or unanticipated harm.
ACA Standard C.2.a: Boundaries of Competence
Counselors practice only within the boundaries of their competence, based on their education, training, supervised experience, state and national professional credentials, and appropriate professional experience. Whereas multicultural counseling competency is required across all counseling specialties, counselors gain knowledge, personal awareness, sensitivity, dispositions, and skills pertinent to being a culturally competent counselor in working with a diverse client population.
ACA Standard A.11.a: Competence Within Termination and Referral
If counselors lack the competence to be of professional assistance to clients, they avoid entering or continuing counseling relationships. Counselors are knowledgeable about culturally and clinically appropriate referral resources and suggest these alternatives. If clients decline the suggested referrals, counselors discontinue the relationship.
ACA Standard A.11.b: Values Within Termination and Referral
Counselors refrain from referring prospective and current clients based solely on the counselor’s personally held values, attitudes, beliefs, and behaviors. Counselors respect the diversity of clients and seek training in areas in which they are at risk of imposing their values onto clients, especially when the counselor’s values are inconsistent with the client’s goals or are discriminatory in nature.
ACA Standard A.11.c: Appropriate Termination
Counselors terminate a counseling relationship when it becomes reasonably apparent that the client no longer needs assistance, is not likely to benefit, or is being harmed by continued counseling. Counselors may terminate counseling when in jeopardy of harm by the client or by another person with whom the client has a relationship, or when clients do not pay fees as agreed upon. Counselors provide pretermination counseling and recommend other service providers when necessary.
ACA Standard A.11.d: Appropriate Transfer of Services
When counselors transfer or refer clients to other practitioners, they ensure that appropriate clinical and administrative processes are completed and open communication is maintained with both clients and practitioners.
National Association of Social Workers (NASW)
NASW Standard 1.01: Commitment to Clients
Social workers’ primary responsibility is to promote the well-being of clients. In general, clients’ interests are primary. However, social workers’ responsibility to the larger society or specific legal obligations may, on limited occasions, supersede the loyalty owed clients, and clients should be so advised. (Examples include when a social worker is required by law to report that a client has abused a child or has threatened to harm self or others.)
NASW Standard 1.04: Competence
(a) Social workers should provide services and represent themselves as competent only within the boundaries of their education, training, license, certification, consultation received, supervised experience, or other relevant professional experience.
(b) Social workers should provide services in substantive areas or use intervention techniques or approaches that are new to them only after engaging in appropriate study, training, consultation, and supervision from people who are competent in those interventions or techniques.
(c) When generally recognized standards do not exist with respect to an emerging area of practice, social workers should exercise careful judgment and take responsible steps (including appropriate education, research, training, consultation, and supervision) to ensure the competence of their work and to protect clients from harm.
(d) Social workers who use technology in the provision of social work services should ensure that they have the necessary knowledge and skills to provide such services in a competent manner. This includes an understanding of the special communication challenges when using technology and the ability to implement strategies to address these challenges.
(e) Social workers who use technology in providing social work services should comply with the laws governing technology and social work practice in the jurisdiction in which they are regulated and located and, as applicable, in the jurisdiction in which the client is located.
NASW Standard 1.16: Referral for Services
(a) Social workers should refer clients to other professionals when the other professionals’ specialized knowledge or expertise is needed to serve clients fully or when social workers believe that they are not being effective or making reasonable progress with clients and that other services are required.
(b) Social workers who refer clients to other professionals should take appropriate steps to facilitate an orderly transfer of responsibility. Social workers who refer clients to other professionals should disclose, with clients’ consent, all pertinent information to the new service providers.
(c) Social workers are prohibited from giving or receiving payment for a referral when no professional service is provided by the referring social worker.
NASW Standard 1.17: Termination of Services
(a) Social workers should terminate services to clients and professional relationships with them when such services and relationships are no longer required or no longer serve the clients’ needs or interests.
(b) Social workers should take reasonable steps to avoid abandoning clients who are still in need of services. Social workers should withdraw services precipitously only under unusual circumstances, giving careful consideration to all factors in the situation and taking care to minimize possible adverse effects. Social workers should assist in making appropriate arrangements for continuation of services when necessary.
(c) Social workers in fee-for-service settings may terminate services to clients who are not paying an overdue balance if the financial contractual arrangements have been made clear to the client, if the client does not pose an imminent danger to self or others, and if the clinical and other consequences of the current nonpayment have been addressed and discussed with the client.
(d) Social workers should not terminate services to pursue a social, financial, or sexual relationship with a client.
(e) Social workers who anticipate the termination or interruption of services to clients should notify clients promptly and seek the transfer, referral, or continuation of services in relation to the clients’ needs and preferences.
(f) Social workers who are leaving an employment setting should inform clients of appropriate options for the continuation of services and of the benefits and risks of the options.
Section 6: Privacy, Confidentiality, Records, and Information Sharing
Dating and relationship services routinely collect sensitive information, photographs, communications, screening results, preferences, and safety information. Providers should collect only information that is reasonably necessary, explain how it will be used, restrict access, use appropriate security safeguards, and retain or dispose of records according to applicable law and policy. Confidentiality obligations may arise from professional ethics, law, contract, platform policy, or a combination of these sources.
A matchmaker often serves two people whose interests may diverge. Before sharing profiles, feedback, screening information, or reasons for declining a match, the provider should define what each person has authorized for disclosure. Information learned privately from one participant should not automatically be disclosed to another. Consultation, teaching, publicity, and testimonials require authorization or effective de-identification. Safety disclosures should be limited to what is legally and ethically necessary.
Applicable ethical guidance.
APA Standards 4.01–4.07 require protection of confidential information, discussion of confidentiality limits, and appropriate authorization or de-identification before disclosure. AAMFT Standard II requires protection of each client’s confidences and careful authorization when information is used outside treatment. ACA Standards B.1.c–B.1.d require respect for confidentiality and explanation of its limits; B.3.e and Section H address secure electronic transmission. NASW Standard 1.07 requires protection of privacy, disclosure only with valid consent or a compelling exception, use of the least information necessary, and safeguards such as encryption, firewalls, and passwords. The provider should obtain specific consent, disclose minimally, and secure both clinical and nonclinical relationship-service data.
Complete cited source text
American Psychological Association (APA)
Standard 4.01: Maintaining Confidentiality
Psychologists have a primary obligation and take reasonable precautions to protect confidential information obtained through or stored in any medium, recognizing that the extent and limits of confidentiality may be regulated by law or established by institutional rules or professional or scientific relationship. (See also Standard 2.05, Delegation of Work to Others.)
Standard 4.02: Discussing the Limits of Confidentiality
(a) Psychologists discuss with persons (including, to the extent feasible, persons who are legally incapable of giving informed consent and their legal representatives) and organizations with whom they establish a scientific or professional relationship (1) the relevant limits of confidentiality and (2) the foreseeable uses of the information generated through their psychological activities. (See also Standard 3.10, Informed Consent.)
(b) Unless it is not feasible or is contraindicated, the discussion of confidentiality occurs at the outset of the relationship and thereafter as new circumstances may warrant.
(c) Psychologists who offer services, products, or information via electronic transmission inform clients/patients of the risks to privacy and limits of confidentiality.
Standard 4.03: Recording
Before recording the voices or images of individuals to whom they provide services, psychologists obtain permission from all such persons or their legal representatives. (See also Standards 8.03, Informed Consent for Recording Voices and Images in Research; 8.05, Dispensing with Informed Consent for Research; and 8.07, Deception in Research.)
Standard 4.04: Minimizing Intrusions on Privacy
(a) Psychologists include in written and oral reports and consultations, only information germane to the purpose for which the communication is made.
(b) Psychologists discuss confidential information obtained in their work only for appropriate scientific or professional purposes and only with persons clearly concerned with such matters.
Standard 4.05: Disclosures
(a) Psychologists may disclose confidential information with the appropriate consent of the organizational client, the individual client/patient, or another legally authorized person on behalf of the client/patient unless prohibited by law.
(b) Psychologists disclose confidential information without the consent of the individual only as mandated by law, or where permitted by law for a valid purpose such as to (1) provide needed professional services; (2) obtain appropriate professional consultations; (3) protect the client/patient, psychologist, or others from harm; or (4) obtain payment for services from a client/patient, in which instance disclosure is limited to the minimum that is necessary to achieve the purpose. (See also Standard 6.04e, Fees and Financial Arrangements.)
Standard 4.06: Consultations
When consulting with colleagues, (1) psychologists do not disclose confidential information that reasonably could lead to the identification of a client/patient, research participant, or other person or organization with whom they have a confidential relationship unless they have obtained the prior consent of the person or organization or the disclosure cannot be avoided, and (2) they disclose information only to the extent necessary to achieve the purposes of the consultation. (See also Standard 4.01, Maintaining Confidentiality.)
Standard 4.07: Use of Confidential Information for Didactic or Other Purposes
Psychologists do not disclose in their writings, lectures, or other public media, confidential, personally identifiable information concerning their clients/patients, students, research participants, organizational clients, or other recipients of their services that they obtained during the course of their work, unless (1) they take reasonable steps to disguise the person or organization, (2) the person or organization has consented in writing, or (3) there is legal authorization for doing so.
American Association for Marriage and Family Therapy (AAMFT)
Standard II: Confidentiality
STANDARD II: CONFIDENTIALITY Marriage and family therapists have unique confidentiality concerns because the client in a therapeutic relationship may be more than one person. Marriage and family therapists respect and guard the confidences of each individual client in the client system.
2.1 Disclosing Limits of Confidentiality. Marriage and family therapists disclose to clients and other parties with a legal interest at the outset of services the nature of confidentiality and possible limitations of the clients’ right to confidentiality. Marriage and family therapists review with clients the circumstances where confidential information may be requested and where disclosure of confidential information may be legally required. Repeated disclosures to clients and other relevant parties may be necessary due to changes in circumstances.
2.2 Written Authorization to Release Client Information. Marriage and family therapists do not disclose client confidences except by written authorization or waiver, or where mandated or permitted by law. Verbal authorization will not be sufficient except in emergency situations, unless prohibited by law. When providing couple, family, or group treatment, the marriage and family therapist does not disclose information outside the treatment context without a written authorization from each individual competent to provide written authorization. In the context of couple, family, or group treatment, the marriage and family therapist must not reveal any individual’s confidences to others in the client unit without the prior written permission of that individual.
2.3 Client Access to Records. Marriage and family therapists provide clients with reasonable access to records concerning the clients. When providing couple, family, or group treatment, the marriage and family therapist does not provide access to records without a written authorization from each individual competent to provide written authorization. Marriage and family therapists limit a client’s access to their records only in exceptional circumstances when there is compelling evidence that such access could cause serious harm to the client. The client’s request and the rationale for withholding some or all of the record must be documented in the client’s file.
Marriage and family therapists take steps to protect the confidentiality of other individuals identified in client records.
2.4 Confidentiality in Non-Clinical Activities. Marriage and family therapists use client and clinical materials in teaching, writing, consulting, research, and public presentations only if written authorization has been obtained in accordance with Standard 2.2, or when appropriate steps have been taken to protect client identity and confidentiality as permitted by law.
2.5 Protection of Records. Marriage and family therapists store, safeguard, and dispose of clinical records to comply with applicable laws and professional standards.
2.6 Breaches. In the event of a breach of clinical records, marriage and family therapists must notify clients in a timely manner that is consistent with applicable laws and professional standards.
2.7 Preparation for Practice Changes. In preparation for moving, selling, or closing a practice, incapacitation, or death, marriage and family therapists arrange for the storage, transfer, or disposal of client records in compliance with applicable laws and professional standards.
2.8 Confidentiality in Consultations. Marriage and family therapists, when consulting with colleagues or referral sources, do not share confidential information that could reasonably lead to the identification of a client, research participant, supervisee, or other person with whom they have a confidential relationship without written authorization. Marriage and family therapists share information only to the extent necessary to achieve the purposes of the consultation.
American Counseling Association (ACA)
ACA Standard B.1.c: Respect for Confidentiality
Counselors protect the confidential information of prospective and current clients. Counselors disclose information only with appropriate consent or with sound legal or ethical justification.
ACA Standard B.1.d: Explanation of Limitations
At initiation and throughout the counseling process, counselors inform clients of the limitations of confidentiality and seek to identify situations in which confidentiality must be breached.
ACA Standard B.3.e: Transmitting Confidential Information
Counselors take precautions to ensure the confidentiality of all information transmitted through the use of any medium.
ACA Section H: Distance Counseling, Technology, and Social Media — Introduction
Counselors understand that the profession of counseling may no longer be limited to in-person, face-to-face interactions. Counselors actively attempt to understand the evolving nature of the profession with regard to distance counseling, technology, and social media and how such resources may be used to better serve their clients. Counselors strive to become knowledgeable about these resources. Counselors understand the additional concerns related to the use of distance counseling, technology, and social media and make every attempt to protect confidentiality and meet any legal and ethical requirements for the use of such resources.
ACA Standard H.1.a: Knowledge and Competency
Counselors who engage in the use of distance counseling, technology, and/or social media develop knowledge and skills regarding related technical, ethical, and legal considerations (e.g., special certifications, additional course work).
ACA Standard H.1.b: Laws and Statutes
Counselors who engage in the use of distance counseling, technology, and social media within their counseling practice understand that they may be subject to laws and regulations of both the counselor’s practicing location and the client’s place of residence. Counselors ensure that their clients are aware of pertinent legal rights and limitations governing the practice of counseling across state lines or international boundaries.
ACA Standard H.2.a: Informed Consent and Disclosure
Clients have the freedom to choose whether to use distance counseling, social media, and/or technology within the counseling process. In addition to the usual and customary protocol of informed consent between counselor and client for face-to-face counseling, the following issues, unique to the use of distance counseling, technology, and/or social media, are addressed in the informed consent process: • distance counseling credentials, physical location of practice, and contact information; • risks and benefits of engaging in the use of distance counseling, technology, and/or social media; • possibility of technology failure and alternate methods of service delivery; • anticipated response time; • emergency procedures to follow when the counselor is not available; • time zone differences; • cultural and/or language differences that may affect delivery of services; • possible denial of insurance benefits; and • social media policy.
ACA Standard H.2.b: Confidentiality Maintained by the Counselor
Counselors acknowledge the limitations of maintaining the confidentiality of electronic records and transmissions. They inform clients that individuals might have authorized or unauthorized access to such records or transmissions (e.g., colleagues, supervisors, employees, information technologists).
ACA Standard H.2.c: Acknowledgment of Limitations
Counselors inform clients about the inherent limits of confidentiality when using technology. Counselors urge clients to be aware of authorized and/or unauthorized access to information disclosed using this medium in the counseling process.
ACA Standard H.2.d: Security
Counselors use current encryption standards within their websites and/or technology-based communications that meet applicable legal requirements. Counselors take reasonable precautions to ensure the confidentiality of information transmitted through any electronic means.
ACA Standard H.3: Client Verification
Counselors who engage in the use of distance counseling, technology, and/or social media to interact with clients take steps to verify the client’s identity at the beginning and throughout the therapeutic process. Verification can include, but is not limited to, using code words, numbers, graphics, or other nondescript identifiers.
ACA Standard H.4.a: Benefits and Limitations
Counselors inform clients of the benefits and limitations of using technology applications in the provision of counseling services. Such technologies include, but are not limited to, computer hardware and/or software, telephones and applications, social media and Internet-based applications and other audio and/or video communication, or data storage devices or media.
ACA Standard H.4.b: Professional Boundaries in Distance Counseling
Counselors understand the necessity of maintaining a professional relationship with their clients. Counselors discuss and establish professional boundaries with clients regarding the appropriate use and/or application of technology and the limitations of its use within the counseling relationship (e.g., lack of confidentiality, times when not appropriate to use).
ACA Standard H.4.c: Technology-Assisted Services
When providing technology-assisted services, counselors make reasonable efforts to determine that clients are intellectually, emotionally, physically, linguistically, and functionally capable of using the application and that the application is appropriate for the needs of the client. Counselors verify that clients understand the purpose and operation of technology applications and follow up with clients to correct possible misconceptions, discover appropriate use, and assess subsequent steps.
ACA Standard H.4.d: Effectiveness of Services
When distance counseling services are deemed ineffective by the counselor or client, counselors consider delivering services face-to-face. If the counselor is not able to provide face-to-face services (e.g., lives in another state), the counselor assists the client in identifying appropriate services.
ACA Standard H.4.e: Access
Counselors provide information to clients regarding reasonable access to pertinent applications when providing technology-assisted services.
ACA Standard H.4.f: Communication Differences in Electronic Media
Counselors consider the differences between face-to-face and electronic communication (nonverbal and verbal cues) and how these may affect the counseling process. Counselors educate clients on how to prevent and address potential misunderstandings arising from the lack of visual cues and voice intonations when communicating electronically.
ACA Standard H.5.a: Records
Counselors maintain electronic records in accordance with relevant laws and statutes. Counselors inform clients on how records are maintained electronically. This includes, but is not limited to, the type of encryption and security assigned to the records, and if/for how long archival storage of transaction records is maintained.
ACA Standard H.5.b: Client Rights
Counselors who offer distance counseling services and/or maintain a professional website provide electronic links to relevant licensure and professional certification boards to protect consumer and client rights and address ethical concerns.
ACA Standard H.5.c: Electronic Links
Counselors regularly ensure that electronic links are working and are professionally appropriate.
ACA Standard H.5.d: Multicultural and Disability Considerations
Counselors who maintain websites provide accessibility to persons with disabilities. They provide translation capabilities for clients who have a different primary language, when feasible. Counselors acknowledge the imperfect nature of such translations and accessibilities.
ACA Standard H.6.a: Virtual Professional Presence
In cases where counselors wish to maintain a professional and personal presence for social media use, separate professional and personal web pages and profiles are created to clearly distinguish between the two kinds of virtual presence.
ACA Standard H.6.b: Social Media as Part of Informed Consent
Counselors clearly explain to their clients, as part of the informed consent procedure, the benefits, limitations, and boundaries of the use of social media.
ACA Standard H.6.c: Client Virtual Presence
Counselors respect the privacy of their clients’ presence on social media unless given consent to view such information.
ACA Standard H.6.d: Use of Public Social Media
Counselors take precautions to avoid disclosing confidential information through public social media.
National Association of Social Workers (NASW)
NASW Standard 1.07: Privacy and Confidentiality
(a) Social workers should respect clients’ right to privacy. Social workers should not solicit private information from or about clients except for compelling professional reasons. Once private information is shared, standards of confidentiality apply.
(b) Social workers may disclose confidential information when appropriate with valid consent from a client or a person legally authorized to consent on behalf of a client.
(c) Social workers should protect the confidentiality of all information obtained in the course of professional service, except for compelling professional reasons. The general
expectation that social workers will keep information confidential does not apply when disclosure is necessary to prevent serious, foreseeable, and imminent harm to a client or others. In all instances, social workers should disclose the least amount of confidential information necessary to achieve the desired purpose; only information that is directly relevant to the purpose for which the disclosure is made should be revealed.
(d) If social workers plan to disclose confidential information, they should (when feasible and to the extent possible) inform clients about the disclosure and the potential consequences prior to disclosing the information. This applies whether social workers disclose confidential information on the basis of a legal requirement or client consent.
(e) Social workers should discuss with clients and other interested parties the nature of confidentiality and limitations of clients’ right to confidentiality. Social workers should review with clients circumstances where confidential information may be requested and where disclosure of confidential information may be legally required. This discussion should occur as soon as possible in the social worker–client relationship and as needed throughout the course of the relationship.
(f) When social workers provide counseling services to families, couples, or groups, social workers should seek agreement among the parties involved concerning each individual’s right to confidentiality and obligation to preserve the confidentiality of information shared by others. This agreement should include consideration of whether confidential information may be exchanged in person or electronically, among clients or with others outside of formal counseling sessions. Social workers should inform participants in family, couples, or group counseling that social workers cannot guarantee that all participants will honor such agreements.
(g) Social workers should inform clients involved in family, couples, marital, or group counseling of the social worker’s, employer’s, and agency’s policy concerning the social worker’s disclosure of confidential information among the parties involved in the counseling.
(h) Social workers should not disclose confidential information to third-party payers unless clients have authorized such disclosure.
(i) Social workers should not discuss confidential information, electronically or in person, in any setting unless privacy can be ensured. Social workers should not discuss confidential information in public or semipublic areas such as hallways, waiting rooms, elevators, and restaurants.
(j) Social workers should protect the confidentiality of clients during legal proceedings to the extent permitted by law. When a court of law or other legally authorized body orders
social workers to disclose confidential or privileged information without a client’s consent and such disclosure could cause harm to the client, social workers should request that the court withdraw the order or limit the order as narrowly as possible or maintain the records under seal, unavailable for public inspection.
(k) Social workers should protect the confidentiality of clients when responding to requests from members of the media.
(l) Social workers should protect the confidentiality of clients’ written and electronic records and other sensitive information. Social workers should take reasonable steps to ensure that clients’ records are stored in a secure location and that clients’ records are not available to others who are not authorized to have access.
(m) Social workers should take reasonable steps to protect the confidentiality of electronic communications, including information provided to clients or third parties. Social workers should use applicable safeguards (such as encryption, firewalls, and passwords) when using electronic communications such as e-mail, online posts, online chat sessions, mobile communication, and text messages.
(n) Social workers should develop and disclose policies and procedures for notifying clients of any breach of confidential information in a timely manner.
(o) In the event of unauthorized access to client records or information, including any unauthorized access to the social worker’s electronic communication or storage systems, social workers should inform clients of such disclosures, consistent with applicable laws and professional standards.
(p) Social workers should develop and inform clients about their policies, consistent with prevailing social work ethical standards, on the use of electronic technology, including Internet-based search engines, to gather information about clients.
(q) Social workers should avoid searching or gathering client information electronically unless there are compelling professional reasons, and when appropriate, with the client’s informed consent.
(r) Social workers should avoid posting any identifying or confidential information about clients on professional Web sites or other forms of social media.
(s) Social workers should transfer or dispose of clients’ records in a manner that protects clients’ confidentiality and is consistent with applicable laws governing records and social work licensure.
(t) Social workers should take reasonable precautions to protect client confidentiality in the event of the social worker’s termination of practice, incapacitation, or death.
(u) Social workers should not disclose identifying information when discussing clients for teaching or training purposes unless the client has consented to disclosure of confidential information.
(v) Social workers should not disclose identifying information when discussing clients with consultants unless the client has consented to disclosure of confidential information or there is a compelling need for such disclosure.
(w) Social workers should protect the confidentiality of deceased clients consistent with the preceding standards.
Section 7: Cultural Responsiveness, Inclusion, and Non-Discrimination
Ethical relationship services recognize that dating goals are shaped by culture, religion, disability, age, race, ethnicity, sexual orientation, gender identity, socioeconomic circumstances, family structure, and relationship traditions. Providers should use inclusive forms and language, seek relevant knowledge, examine their own biases, and avoid stereotyping.
A client retains autonomy over attraction and partner selection, but a provider should not reinforce demeaning stereotypes or operate discriminatory eligibility rules that violate law or professional obligations. When the provider lacks cultural knowledge, consultation, training, or referral may be appropriate. Cultural humility requires treating the client as an expert on their lived experience while retaining responsibility for competent and nondiscriminatory practice.
Applicable ethical guidance.
APA Principle E and Standard 3.01 address respect for individual and cultural differences and prohibit unfair discrimination. AAMFT Standard 1.1 prohibits discrimination in professional assistance. ACA’s preamble emphasizes dignity, diversity, justice, and a multicultural approach, while Standard C.5 prohibits discrimination. NASW Standards 1.05 and 4.02 require cultural competence, cultural humility, self-correction of bias, and rejection of discriminatory practice. Applied to dating services, the provider should respect individual partner preferences without adopting stereotypes, exclusionary practices, or value judgments that compromise equal and respectful service.
Complete cited source text
American Psychological Association (APA)
Principle E: Respect for People’s Rights and Dignity
Psychologists respect the dignity and worth of all people, and the rights of individuals to privacy, confidentiality, and self-determination. Psychologists are aware that special safeguards may be necessary to protect the rights and welfare of persons or communities whose vulnerabilities impair autonomous decision making. Psychologists are aware of and respect cultural, individual, and role differences, including those based on age, gender, gender identity, race, ethnicity, culture, national origin, religion, sexual orientation, disability, language, and socioeconomic status, and consider these factors when working with members of such groups. Psychologists try to eliminate the effect on their work of biases based on those factors, and they do not knowingly participate in or condone activities of others based upon such prejudices.
Standard 3.01: Unfair Discrimination
In their work-related activities, psychologists do not engage in unfair discrimination based on age, gender, gender identity, race, ethnicity, culture, national origin, religion, sexual orientation, disability, socioeconomic status, or any basis proscribed by law.
American Association for Marriage and Family Therapy (AAMFT)
AAMFT Standard 1.1
1.1 Non-Discrimination. Marriage and family therapists provide professional assistance to persons without discrimination on the basis of race/ethnicity, color, religion, national origin, location, citizenship status, sex (including pregnancy, childbirth, and related medical conditions), sexual orientation, sexual or gender expression, gender identity, disability (physical or mental), age, genetic information, marital status, veteran or military status, or any other characteristic protected by applicable law.
American Counseling Association (ACA)
ACA Code of Ethics Preamble — Core Professional Values
Professional values are an important way of living out an ethical commitment. The following are core professional values of the counseling profession: 1. enhancing human development throughout the life span; 2. honoring diversity and embracing a multicultural approach in support of the worth, dignity, potential, and uniqueness of people within their social and cultural contexts; 3. promoting social justice; 4. safeguarding the integrity of the counselor–client relationship; and 5. practicing in a competent and ethical manner.
ACA Code of Ethics Preamble — Fundamental Principles
These professional values provide a conceptual basis for the ethical principles enumerated below. These principles are the foundation for ethical behavior and decision making. The fundamental principles of professional ethical behavior are • autonomy, or fostering the right to control the direction of one’s life; • nonmaleficence, or avoiding actions that cause harm; • beneficence, or working for the good of the individual and society by promoting mental health and well-being; • justice, or treating individuals equitably and fostering fairness and equality; • fidelity, or honoring commitments and keeping promises, including fulfilling one’s responsibilities of trust in professional relationships; and • veracity, or dealing truthfully with individuals with whom counselors come into professional contact.
ACA Standard C.5: Nondiscrimination
Counselors do not condone or engage in discrimination against prospective or current clients, students, employees, supervisees, or research participants based on age, culture, disability, ethnicity, race, religion/spirituality, gender, gender identity, sexual orientation, marital/partnership status, language preference, socioeconomic status, immigration status, or any basis proscribed by law.
National Association of Social Workers (NASW)
NASW Standard 1.05: Cultural Competence
(a) Social workers should demonstrate understanding of culture and its function in human behavior and society, recognizing the strengths that exist in all cultures.
(b) Social workers should demonstrate knowledge that guides practice with clients of various cultures and be able to demonstrate skills in the provision of culturally informed services that empower marginalized individuals and groups. Social workers must take action against oppression, racism, discrimination, and inequities, and acknowledge personal privilege.
(c) Social workers should demonstrate awareness and cultural humility by engaging in critical self-reflection (understanding their own bias and engaging in self-correction), recognizing clients as experts of their own culture, committing to lifelong learning, and holding institutions accountable for advancing cultural humility.
(d) Social workers should obtain education about and demonstrate understanding of the nature of social diversity and oppression with respect to race, ethnicity, national origin, color, sex, sexual orientation, gender identity or expression, age, marital status, political belief, religion, immigration status, and mental or physical ability.
(e) Social workers who provide electronic social work services should be aware of cultural and socioeconomic differences among clients’ use of and access to electronic technology and seek to prevent such potential barriers. Social workers should assess cultural, environmental, economic, mental or physical ability, linguistic, and other issues that may affect the delivery or use of these services.
NASW Standard 4.02: Discrimination
Social workers should not practice, condone, facilitate, or collaborate with any form of discrimination on the basis of race, ethnicity, national origin, color, sex, sexual orientation, gender identity or expression, age, marital status, political belief, religion, immigration status, or mental or physical ability.
Section 8: Boundaries, Multiple Roles, Sexual Relationships, and Conflicts of Interest
The informality of coaching and matchmaking can obscure the power differential created by access to intimate information, the promise of connection, and the provider’s influence over introductions. Providers should maintain clear professional boundaries and avoid relationships that impair judgment, create divided loyalty, or increase the risk of exploitation.
A provider should not date, pursue, or engage sexually with a current client or matchmaking participant under the provider’s care. Licensed clinicians must follow the stricter rules applicable to their profession, including restrictions that may continue after termination. Business partnerships, employment, investments, gifts, social-media relationships, and personal friendships require careful assessment. In a small community, incidental contact may be unavoidable, but confidentiality and role clarity remain essential.
Applicable ethical guidance.
APA Standards 3.05 and 10.05–10.08 address multiple relationships and sexual relationships with therapy clients or former clients. AAMFT Standards 1.6 and the Code’s sexual-intimacy provisions prohibit abuse of the therapeutic relationship. ACA Standards A.5.a–A.5.c prohibit sexual or romantic relationships with current clients and impose restrictions concerning former clients; A.6 requires careful management of boundary extensions. NASW Standards 1.06 and 1.09 prohibit exploitative conflicts and sexual relationships with current clients and restrict relationships with former clients. The safest operational rule is that no provider should use a professional relationship or matchmaking access to pursue personal, sexual, financial, or social benefit.
Complete cited source text
American Psychological Association (APA)
Standard 3.05: Multiple Relationships
(a) A multiple relationship occurs when a psychologist is in a professional role with a person and (1) at the same time is in another role with the same person, (2) at the same time is in a relationship with a person closely associated with or related to the person with whom the psychologist has the professional relationship, or (3) promises to enter into another relationship in the future with the person or a person closely associated with or related to the person. A psychologist refrains from entering into a multiple relationship if the multiple relationship could reasonably be expected to impair the psychologist’s objectivity, competence, or effectiveness in performing his or her functions as a psychologist, or otherwise risks exploitation or harm to the person with whom the professional relationship exists. Multiple relationships that would not reasonably be expected to cause impairment or risk exploitation or harm are not unethical.
(b) If a psychologist finds that, due to unforeseen factors, a potentially harmful multiple relationship has arisen, the psychologist takes reasonable steps to resolve it with due regard for the best interests of the affected person and maximal compliance with the Ethics Code.
(c) When psychologists are required by law, institutional policy, or extraordinary circumstances to serve in more than one role in judicial or administrative proceedings, at the outset they clarify role expectations and the extent of confidentiality and thereafter as changes occur. (See also Standards 3.04, Avoiding Harm, and 3.07, Third-Party Requests for Services.)
Standard 10.05: Sexual Intimacies with Current Therapy Clients/Patients
Psychologists do not engage in sexual intimacies with current therapy clients/patients.
Standard 10.06: Sexual Intimacies with Relatives or Significant Others of Current Therapy Clients/Patients
Psychologists do not engage in sexual intimacies with individuals they know to be close relatives, guardians, or significant others of current clients/patients. Psychologists do not terminate therapy to circumvent this standard.
Standard 10.07: Therapy with Former Sexual Partners
Psychologists do not accept as therapy clients/patients persons with whom they have engaged in sexual intimacies.
Standard 10.08: Sexual Intimacies with Former Therapy Clients/Patients
(a) Psychologists do not engage in sexual intimacies with former clients/patients for at least two years after cessation or termination of therapy.
(b) Psychologists do not engage in sexual intimacies with former clients/patients even after a two-year interval except in the most unusual circumstances. Psychologists who engage in such activity after the two years following cessation or termination of therapy and of having no sexual contact with the former client/patient bear the burden of demonstrating that there has been no exploitation, in light of all relevant factors, including (1) the amount of time that has passed since therapy terminated; (2) the nature, duration, and intensity of the therapy; (3) the circumstances of termination; (4) the client’s/patient’s personal history; (5) the client’s/patient’s current mental status; (6) the likelihood of adverse impact on the client/patient; and (7) any statements or actions made by the therapist during the course of therapy suggesting or inviting the possibility of a posttermination sexual or romantic relationship with the client/patient. (See also Standard 3.05, Multiple Relationships.)
American Association for Marriage and Family Therapy (AAMFT)
AAMFT Standard 1.6
1.6 Abuse of the Therapeutic Relationship. Marriage and family therapists do not abuse their power in therapeutic relationships.
AAMFT Standard 1.4
1.4 Sexual Behavior with Current Clients, Former Clients, and Others. All forms of sexual behavior with current and former clients or with known members of the client’s family system are prohibited.
American Counseling Association (ACA)
ACA Standard A.5.a: Sexual and/or Romantic Relationships Prohibited
Sexual and/or romantic counselor–client interactions or relationships with current clients, their romantic partners, or their family members are prohibited. This prohibition applies to both in-person and electronic interactions or relationships.
ACA Standard A.5.b: Previous Sexual and/or Romantic Relationships
Counselors are prohibited from engaging in counseling relationships with persons with whom they have had a previous sexual and/or romantic relationship.
ACA Standard A.5.c: Sexual and/or Romantic Relationships With Former Clients
Sexual and/or romantic counselor–client interactions or relationships with former clients, their romantic partners, or their family members are prohibited for a period of 5 years following the last professional contact. This prohibition applies to both in-person and electronic interactions or relationships. Counselors, before engaging in sexual and/or romantic interactions or relationships with former clients, their romantic partners, or their family members, demonstrate forethought and document (in written form) whether the interaction or relationship can be viewed as exploitive in any way and/or whether there is still potential to harm the former client; in cases of potential exploitation and/or harm, the counselor avoids entering into such an interaction or relationship.
ACA Standard A.6.a: Previous Relationships
Counselors consider the risks and benefits of accepting as clients those with whom they have had a previous relationship. These potential clients may include individuals with whom the counselor has had a casual, distant, or past relationship. Examples include mutual or past membership in a professional association, organization, or community. When counselors accept these clients, they take appropriate professional precautions such as informed consent, consultation, supervision, and documentation to ensure that judgment is not impaired and no exploitation occurs.
ACA Standard A.6.b: Extending Counseling Boundaries
Counselors consider the risks and benefits of extending current counseling relationships beyond conventional parameters. Examples include attending a client’s formal ceremony (e.g., a wedding/commitment ceremony or graduation), purchasing a service or product provided by a client (excepting unrestricted bartering), and visiting a client’s ill family member in the hospital. In extending these boundaries, counselors take appropriate professional precautions such as informed consent, consultation, supervision, and documentation to ensure that judgment is not impaired and no harm occurs.
ACA Standard A.6.c: Documenting Boundary Extensions
If counselors extend boundaries as described in A.6.a. and A.6.b., they must officially document, prior to the interaction (when feasible), the rationale for such an interaction, the potential benefit, and anticipated consequences for the client or former client and other individuals significantly involved with the client or former client. When unintentional harm occurs to the client or former client, or to an individual significantly involved with the client or former client, the counselor must show evidence of an attempt to remedy such harm.
ACA Standard A.6.d: Role Changes in the Professional Relationship
When counselors change a role from the original or most recent contracted relationship, they obtain informed consent from the client and explain the client’s right to refuse services related to the change. Examples of role changes include, but are not limited to 1. changing from individual to relationship or family counseling, or vice versa; 2. changing from an evaluative role to a therapeutic role, or vice versa; and 3. changing from a counselor to a mediator role, or vice versa. Clients must be fully informed of any anticipated consequences (e.g., financial, legal, personal, therapeutic) of counselor role changes.
ACA Standard A.6.e: Nonprofessional Interactions or Relationships (Other Than Sexual or Romantic Interactions or Relationships)
Counselors avoid entering into nonprofessional relationships with former clients, their romantic partners, or their family members when the interaction is potentially harmful to the client. This applies to both in-person and electronic interactions or relationships.
National Association of Social Workers (NASW)
NASW Standard 1.06: Conflicts of Interest
(a) Social workers should be alert to and avoid conflicts of interest that interfere with the exercise of professional discretion and impartial judgment. Social workers should inform clients when a real or potential conflict of interest arises and take reasonable steps to resolve the issue in a manner that makes the clients’ interests primary and protects clients’ interests to the greatest extent possible. In some cases, protecting clients’ interests may require termination of the professional relationship with proper referral of the client.
(b) Social workers should not take unfair advantage of any professional relationship or exploit others to further their personal, religious, political, or business interests.
(c) Social workers should not engage in dual or multiple relationships with clients or former clients in which there is a risk of exploitation or potential harm to the client. In instances when dual or multiple relationships are unavoidable, social workers should take steps to protect clients and are responsible for setting clear, appropriate, and culturally sensitive boundaries. (Dual or multiple relationships occur when social workers relate to clients in
more than one relationship, whether professional, social, or business. Dual or multiple relationships can occur simultaneously or consecutively.)
(d) When social workers provide services to two or more people who have a relationship with each other (for example, couples, family members), social workers should clarify with all parties which individuals will be considered clients and the nature of social workers’ professional obligations to the various individuals who are receiving services. Social workers who anticipate a conflict of interest among the individuals receiving services or who anticipate having to perform in potentially conflicting roles (for example, when a social worker is asked to testify in a child custody dispute or divorce proceedings involving clients) should clarify their role with the parties involved and take appropriate action to minimize any conflict of interest.
(e) Social workers should avoid communication with clients using technology (such as social networking sites, online chat, e-mail, text messages, telephone, and video) for personal or non-work-related purposes.
(f) Social workers should be aware that posting personal information on professional Web sites or other media might cause boundary confusion, inappropriate dual relationships, or harm to clients.
(g) Social workers should be aware that personal affiliations may increase the likelihood that clients may discover the social worker’s presence on Web sites, social media, and other forms of technology. Social workers should be aware that involvement in electronic communication with groups based on race, ethnicity, language, sexual orientation, gender identity or expression, mental or physical ability, religion, immigration status, and other personal affiliations may affect their ability to work effectively with particular clients.
(h) Social workers should avoid accepting requests from or engaging in personal relationships with clients on social networking sites or other electronic media to prevent boundary confusion, inappropriate dual relationships, or harm to clients.
NASW Standard 1.09: Sexual Relationships
(a) Social workers should under no circumstances engage in sexual activities, inappropriate sexual communications through the use of technology or in person, or sexual contact with current clients, whether such contact is consensual or forced.
(b) Social workers should not engage in sexual activities or sexual contact with clients’ relatives or other individuals with whom clients maintain a close personal relationship when there is a risk of exploitation or potential harm to the client. Sexual activity or sexual contact with clients’ relatives or other individuals with whom clients maintain a personal relationship has the potential to be harmful to the client and may make it difficult for the
social worker and client to maintain appropriate professional boundaries. Social workers— not their clients, their clients’ relatives, or other individuals with whom the client maintains a personal relationship—assume the full burden for setting clear, appropriate, and culturally sensitive boundaries.
(c) Social workers should not engage in sexual activities or sexual contact with former clients because of the potential for harm to the client. If social workers engage in conduct contrary to this prohibition or claim that an exception to this prohibition is warranted because of extraordinary circumstances, it is social workers—not their clients—who assume the full burden of demonstrating that the former client has not been exploited, coerced, or manipulated, intentionally or unintentionally.
(d) Social workers should not provide clinical services to individuals with whom they have had a prior sexual relationship. Providing clinical services to a former sexual partner has the potential to be harmful to the individual and is likely to make it difficult for the social worker and individual to maintain appropriate professional boundaries.
Section 9: Insurance Billing, Clinical Documentation, and Separation of Services
Insurance claims must represent medically necessary covered services actually provided. Dating advice, introductions, profile development, social-event participation, image consulting, and general coaching are not converted into psychotherapy merely because a licensed clinician provides them. A psychotherapy claim should be supported by a clinically appropriate diagnosis, treatment purpose, service, time, and record consistent with payer requirements and applicable law.
When a clinician provides both psychotherapy and private-pay coaching, the services should be differentiated through informed consent, scheduling, documentation, fees, records, and communications. The clinician should not bill insurance for noncovered coaching, divide one encounter artificially, or use a clinical diagnosis solely to secure reimbursement. Referrals from a dating platform should not create pressure to diagnose, prolong treatment, or share protected information without authorization.
Applicable ethical guidance.
APA Standards 5.01, 6.04, and 6.06 require accurate statements, fee clarity, and accurate reporting to payers. AAMFT’s financial integrity standards prohibit misrepresentation in billing. ACA Standards C.6.b and A.10 address accurate reports and financial arrangements. NASW Standards 3.05 and 4.04 require accurate billing and prohibit dishonesty, fraud, or deception. The ethical rule is exact correspondence among the service delivered, the service described to the client, the documentation created, and the service billed.
Complete cited source text
American Psychological Association (APA)
Standard 5.01: Avoidance of False or Deceptive Statements
(a) Public statements include but are not limited to paid or unpaid advertising, product endorsements, grant applications, licensing applications, other credentialing applications, brochures, printed matter, directory listings, personal resumes or curricula vitae, or comments for use in media such as print or electronic transmission, statements in legal proceedings, lectures and public oral presentations, and published materials. Psychologists do not knowingly make public statements that are false, deceptive, or fraudulent concerning their research, practice, or other work activities or those of persons or organizations with which they are affiliated.
(b) Psychologists do not make false, deceptive, or fraudulent statements concerning (1) their training, experience, or competence; (2) their academic degrees; (3) their credentials; (4) their institutional or association affiliations; (5) their services; (6) the scientific or clinical basis for, or results or degree of success of, their services; (7) their fees; or (8) their publications or research findings.
(c) Psychologists claim degrees as credentials for their health services only if those degrees (1) were earned from a regionally accredited educational institution or (2) were the basis for psychology licensure by the state in which they practice.
Standard 6.04: Fees and Financial Arrangements
(a) As early as is feasible in a professional or scientific relationship, psychologists and recipients of psychological services reach an agreement specifying compensation and billing arrangements.
(b) Psychologists’ fee practices are consistent with law.
(c) Psychologists do not misrepresent their fees.
(d) If limitations to services can be anticipated because of limitations in financing, this is discussed with the recipient of services as early as is feasible. (See also Standards 10.09, Interruption of Therapy, and 10.10, Terminating Therapy.)
(e) If the recipient of services does not pay for services as agreed, and if psychologists intend to use collection agencies or legal measures to collect the fees, psychologists first inform the person that such measures will be taken and provide that person an opportunity to make prompt payment. (See also Standards 4.05, Disclosures; 6.03, Withholding Records for Nonpayment; and 10.01, Informed Consent to Therapy.)
Standard 6.06: Accuracy in Reports to Payors and Funding Sources
In their reports to payors for services or sources of research funding, psychologists take reasonable steps to ensure the accurate reporting of the nature of the service provided or research conducted, the fees, charges, or payments, and where applicable, the identity of the provider, the findings, and the diagnosis. (See also Standards 4.01, Maintaining Confidentiality; 4.04, Minimizing Intrusions on Privacy; and 4.05, Disclosures.)
American Association for Marriage and Family Therapy (AAMFT)
Standard VIII: Financial Arrangements
STANDARD VIII: FINANCIAL ARRANGEMENTS Marriage and family therapists make financial arrangements with clients, third-party payors, and supervisees that are reasonably understandable and conform to accepted professional practices and applicable laws.
8.1 Financial Integrity. Marriage and family therapists do not offer or accept kickbacks, rebates, bonuses, or other remuneration for referrals.
8.2 Disclosure of Financial Policies. Prior to entering into the therapeutic or supervisory relationship, marriage and family therapists clearly disclose and explain to clients and supervisees in writing: (a) all financial arrangements and fees related to professional services, including charges for canceled or missed appointments; (b) the use of collection agencies or legal measures for nonpayment; and (c) the policy of obtaining payment from the client, to the extent allowed by law, if payment is denied by the third-party payor. Once services have begun, therapists provide reasonable notice of any changes in fees or other charges.
8.3 Notice of Payment Recovery Procedures. Marriage and family therapists give reasonable notice to clients with unpaid balances of their intent to seek collection by agency or legal recourse. When such action is taken, marriage and family therapists will not disclose clinical information unless permitted or mandated by law.
8.4 Truthful Representation of Services. Marriage and family therapists represent facts truthfully to clients, third-party payors, and supervisees regarding services rendered.
8.5 Bartering. Marriage and family therapists ordinarily refrain from accepting goods and services from clients in return for services rendered. Bartering for professional services may be conducted only if: (a) the supervisee or client requests it; (b) the relationship is not exploitative; (c) the professional relationship is not distorted; (d) a clear written contract is established; and (e) the marriage and family therapist documents the rationale for entering into the bartering agreement.
8.6 Withholding Records for Non-Payment. Marriage and family therapists may not withhold records under their immediate control solely because payment has not been received for past services.
American Counseling Association (ACA)
ACA Standard C.6.b: Reports to Third Parties
Counselors are accurate, honest, and objective in reporting their professional activities and judgments to appropriate third parties, including courts, health insurance companies, those who are the recipients of evaluation reports, and others.
ACA Standard A.10.a: Self-Referral
Counselors working in an organization (e.g., school, agency, institution) that provides counseling services do not refer clients to their private practice unless the policies of a particular organization make explicit provisions for self-referrals. In such instances, the clients must be informed of other options open to them should they seek private counseling services.
ACA Standard A.10.b: Unacceptable Business Practices
Counselors do not participate in fee splitting, nor do they give or receive commissions, rebates, or any other form of remuneration when referring clients for professional services.
ACA Standard A.10.c: Establishing Fees
In establishing fees for professional counseling services, counselors consider the financial status of clients and locality. If a counselor’s usual fees create undue hardship for the client, the counselor may adjust fees, when legally permissible, or assist the client in locating comparable, affordable services.
ACA Standard A.10.d: Nonpayment of Fees
If counselors intend to use collection agencies or take legal measures to collect fees from clients who do not pay for services as agreed upon, they include such information in their informed consent documents and also inform clients in a timely fashion of intended actions and offer clients the opportunity to make payment.
ACA Standard A.10.e: Bartering
Counselors may barter only if the bartering does not result in exploitation or harm, if the client requests it, and if such arrangements are an accepted practice among professionals in the community. Counselors consider the cultural implications of bartering and discuss relevant concerns with clients and document such agreements in a clear written contract.
ACA Standard A.10.f: Receiving Gifts
Counselors understand the challenges of accepting gifts from clients and recognize that in some cultures, small gifts are a token of respect and gratitude. When determining whether to accept a gift from clients, counselors take into account the therapeutic relationship, the monetary value of the gift, the client’s motivation for giving the gift, and the counselor’s motivation for wanting to accept or decline the gift.
National Association of Social Workers (NASW)
NASW Standard 3.05: Billing
Social workers should establish and maintain billing practices that accurately reflect the nature and extent of services provided and that identify who provided the service in the practice setting.
NASW Standard 4.04: Dishonesty, Fraud, and Deception
Social workers should not participate in, condone, or be associated with dishonesty, fraud, or deception.
Section 10: Consultation, Complaints, Continuing Competence, and Ending Services
Providers should maintain a process for ethical decision-making, consultation, complaints, correction of errors, continuity of services, and termination. Novel services involving platforms, screening tools, artificial intelligence, or combined clinical and nonclinical roles require additional education and periodic review. Consultation should protect confidentiality and should not be used to transfer responsibility for the final decision.
Services should end when goals are met, the client no longer benefits, the service is no longer appropriate, or the provider cannot continue competently. Providers should avoid fostering dependency or extending services primarily for financial gain. When termination may create risk, reasonable transition planning and referral should be provided.
Applicable ethical guidance.
APA Principle B emphasizes professional responsibility and consultation; Standards 10.09–10.10 address interruption and termination. AAMFT’s 2026 Code expressly encourages consultation when ethical questions are uncertain and requires adherence to the higher ethical standard when it exceeds law. ACA Standards C.2.f–C.2.g address continuing competence and impairment, while Section I requires a credible ethical decision-making process. NASW Standards 1.15–1.17 and 4.01 require continuity, referral, responsible termination, and continuing competence. Providers should document the reasoning supporting difficult decisions and be able to explain why the decision protected client welfare and public trust.
American Psychological Association (APA)
Principle B: Fidelity and Responsibility
Psychologists establish relationships of trust with those with whom they work. They are aware of their professional and scientific responsibilities to society and to the specific communities in which they work. Psychologists uphold professional standards of conduct, clarify their professional roles and obligations, accept appropriate responsibility for their behavior, and seek to manage conflicts of interest that could lead to exploitation or harm. Psychologists consult with, refer to, or cooperate with other professionals and institutions to the extent needed to serve the best interests of those with whom they work. They are concerned about the ethical compliance of their colleagues’ scientific and professional conduct. Psychologists strive to contribute a portion of their professional time for little or no compensation or personal advantage.
Standard 10.09: Interruption of Therapy
When entering into employment or contractual relationships, psychologists make reasonable efforts to provide for orderly and appropriate resolution of responsibility for client/patient care in the event that the employment or contractual relationship ends, with paramount consideration given to the welfare of the client/patient. (See also Standard 3.12, Interruption of Psychological Services.)
Standard 10.10: Terminating Therapy
(a) Psychologists terminate therapy when it becomes reasonably clear that the client/patient no longer needs the service, is not likely to benefit, or is being harmed by continued service.
(b) Psychologists may terminate therapy when threatened or otherwise endangered by the client/patient or another person with whom the client/patient has a relationship.
(c) Except where precluded by the actions of clients/patients or third-party payors, prior to termination psychologists provide pretermination counseling and suggest alternative service providers as appropriate.
American Association for Marriage and Family Therapy (AAMFT)
AAMFT Code of Ethics — Seeking Consultation
Seeking Consultation Although the AAMFT Code of Ethics seeks to be comprehensive, it is not exhaustive and there may be behaviors or situations that implicate ethical principles but are not explicitly addressed here. Marriage and family therapists who are uncertain about the ethics of a particular course of action are encouraged to seek counsel from consultants, attorneys, supervisors, colleagues, or other appropriate authorities.
AAMFT Code of Ethics — Ethical Decision-Making
Ethical Decision-Making Both law and ethics govern the practice of marriage and family therapy. When making decisions regarding professional behavior, marriage and family therapists must consider the AAMFT Code of Ethics and applicable laws and regulations. If the AAMFT Code of Ethics prescribes a standard higher than that required by law, marriage and family therapists must meet the higher standard of the AAMFT Code of Ethics. Marriage and family therapists comply with the mandates of law, clearly communicate their commitment to the AAMFT Code of Ethics, and take steps to resolve the conflict in a responsible manner. The AAMFT supports legal mandates for reporting of alleged unethical conduct.
Marriage and family therapists remain accountable to the AAMFT Code of Ethics when acting as members or employees of organizations. If the mandates of an organization with which a marriage and family therapist is affiliated, through employment, contract or otherwise, conflict with the AAMFT Code of Ethics, marriage and family therapists clearly communicate to the organization their commitment to the AAMFT Code of Ethics and take reasonable steps to resolve the conflict in a way that allows the fullest adherence to the Code of Ethics.
American Counseling Association (ACA)
ACA Standard C.2.f: Continuing Education
Counselors recognize the need for continuing education to acquire and maintain a reasonable level of awareness of current scientific and professional information in their fields of activity. Counselors maintain their competence in the skills they use, are open to new procedures, and remain informed regarding best practices for working with diverse populations.
ACA Standard C.2.g: Impairment
Counselors monitor themselves for signs of impairment from their own physical, mental, or emotional problems and refrain from offering or providing professional services when impaired. They seek assistance for problems that reach the level of professional impairment, and, if necessary, they limit, suspend, or terminate their professional responsibilities until it is determined that they may safely resume their work. Counselors assist colleagues or supervisors in recognizing their own professional impairment and provide consultation and assistance when warranted with colleagues or supervisors showing signs of impairment and intervene as appropriate to prevent imminent harm to clients.
ACA Section I: Resolving Ethical Issues — Introduction
Professional counselors behave in an ethical and legal manner. They are aware that client welfare and trust in the profession depend on a high level of professional conduct. They hold other counselors to the same standards and are willing to take appropriate action to ensure that standards are upheld. Counselors strive to resolve ethical dilemmas with direct and open communication among all parties involved and seek consultation with colleagues and supervisors when necessary. Counselors incorporate ethical practice into their daily professional work and engage in ongoing professional development regarding current topics in ethical and legal issues in counseling. Counselors become familiar with the ACA Policy and Procedures for Processing Complaints of Ethical Violations and use it as a reference for assisting in the enforcement of the ACA Code of Ethics.
ACA Standard I.1.a: Knowledge
Counselors know and understand the ACA Code of Ethics and other applicable ethics codes from professional organizations or certification and licensure bodies of which they are members. Lack of knowledge or misunderstanding of an ethical responsibility is not a defense against a charge of unethical conduct.
ACA Standard I.1.b: Ethical Decision Making
When counselors are faced with an ethical dilemma, they use and document, as appropriate, an ethical decision-making model that may include, but is not limited to, consultation; consideration of relevant ethical standards, principles, and laws; generation of potential courses of action; deliberation of risks and benefits; and selection of an objective decision based on the circumstances and welfare of all involved.
ACA Standard I.1.c: Conflicts Between Ethics and Laws
If ethical responsibilities conflict with the law, regulations, and/or other governing legal authority, counselors make known their commitment to the ACA Code of Ethics and take steps to resolve the conflict. If the conflict cannot be resolved using this approach, counselors, acting in the best interest of the client, may adhere to the requirements of the law, regulations, and/or other governing legal authority.
ACA Standard I.2.a: Informal Resolution
When counselors have reason to believe that another counselor is violating or has violated an ethical standard and substantial harm has not occurred, they attempt to first resolve the issue informally with the other counselor if feasible, provided such action does not violate confidentiality rights that may be involved.
ACA Standard I.2.b: Reporting Ethical Violations
If an apparent violation has substantially harmed or is likely to substantially harm a person or organization and is not appropriate for informal resolution or is not resolved properly, counselors take further action depending on the situation. Such action may include referral to state or national committees on professional ethics, voluntary national certification bodies, state licensing boards, or appropriate institutional authorities. The confidentiality rights of clients should be considered in all actions. This standard does not apply when counselors have been retained to review the work of another counselor whose professional conduct is in question (e.g., consultation, expert testimony).
ACA Standard I.2.c: Consultation
When uncertain about whether a particular situation or course of action may be in violation of the ACA Code of Ethics, counselors consult with other counselors who are knowledgeable about ethics and the ACA Code of Ethics, with colleagues, or with appropriate authorities, such as the ACA Ethics and Professional Standards Department.
ACA Standard I.2.d: Organizational Conflicts
If the demands of an organization with which counselors are affiliated pose a conflict with the ACA Code of Ethics, counselors specify the nature of such conflicts and express to their supervisors or other responsible officials their commitment to the ACA Code of Ethics and, when possible, work through the appropriate channels to address the situation.
ACA Standard I.2.e: Unwarranted Complaints
Counselors do not initiate, participate in, or encourage the filing of ethics complaints that are retaliatory in nature or are made with reckless disregard or willful ignorance of facts that would disprove the allegation.
ACA Standard I.2.f: Unfair Discrimination Against Complainants and Respondents
Counselors do not deny individuals employment, advancement, admission to academic or other programs, tenure, or promotion based solely on their having made or their being the subject of an ethics complaint. This does not preclude taking action based on the outcome of such proceedings or considering other appropriate information.
ACA Standard I.3: Cooperation With Ethics Committees
Counselors assist in the process of enforcing the ACA Code of Ethics. Counselors cooperate with investigations, proceedings, and requirements of the ACA Ethics Committee or ethics committees of other duly constituted associations or boards having jurisdiction over those charged with a violation.
National Association of Social Workers (NASW)
NASW Standard 1.15: Interruption of Services
Social workers should make reasonable efforts to ensure continuity of services in the event that services are interrupted by factors such as unavailability, disruptions in electronic communication, relocation, illness, mental or physical ability, or death.
NASW Standard 1.16: Referral for Services
(a) Social workers should refer clients to other professionals when the other professionals’ specialized knowledge or expertise is needed to serve clients fully or when social workers believe that they are not being effective or making reasonable progress with clients and that other services are required.
(b) Social workers who refer clients to other professionals should take appropriate steps to facilitate an orderly transfer of responsibility. Social workers who refer clients to other professionals should disclose, with clients’ consent, all pertinent information to the new service providers.
(c) Social workers are prohibited from giving or receiving payment for a referral when no professional service is provided by the referring social worker.
NASW Standard 1.17: Termination of Services
(a) Social workers should terminate services to clients and professional relationships with them when such services and relationships are no longer required or no longer serve the clients’ needs or interests.
(b) Social workers should take reasonable steps to avoid abandoning clients who are still in need of services. Social workers should withdraw services precipitously only under unusual circumstances, giving careful consideration to all factors in the situation and taking care to minimize possible adverse effects. Social workers should assist in making appropriate arrangements for continuation of services when necessary.
(c) Social workers in fee-for-service settings may terminate services to clients who are not paying an overdue balance if the financial contractual arrangements have been made clear to the client, if the client does not pose an imminent danger to self or others, and if the clinical and other consequences of the current nonpayment have been addressed and discussed with the client.
(d) Social workers should not terminate services to pursue a social, financial, or sexual relationship with a client.
(e) Social workers who anticipate the termination or interruption of services to clients should notify clients promptly and seek the transfer, referral, or continuation of services in relation to the clients’ needs and preferences.
(f) Social workers who are leaving an employment setting should inform clients of appropriate options for the continuation of services and of the benefits and risks of the options.
NASW Standard 4.01: Competence
(a) Social workers should accept responsibility or employment only on the basis of existing competence or the intention to acquire the necessary competence.
(b) Social workers should strive to become and remain proficient in professional practice and the performance of professional functions. Social workers should critically examine and keep current with emerging knowledge relevant to social work. Social workers should
routinely review the professional literature and participate in continuing education relevant to social work practice and social work ethics.
(c) Social workers should base practice on recognized knowledge, including empirically based knowledge, relevant to social work and social work ethics.
Integrated Ethical Standard for Dating and Relationship Services
Across APA, AAMFT, ACA, and NASW, a consistent multidisciplinary standard emerges: providers must place client welfare first; respect informed choice; practice within competence; describe credentials, services, outcomes, and fees truthfully; protect privacy; avoid exploitation and conflicting roles; provide culturally responsive and nondiscriminatory services; maintain accurate records and billing; seek consultation when necessary; and refer or terminate responsibly. These duties apply directly to licensed professionals when required by their governing code, board rules, employment, or contract. They also provide a defensible minimum benchmark for nonlicensed coaches and matchmakers who handle vulnerable clients and highly sensitive information.
Professional Ethical Codes
American Psychological Association. (2002). Ethical Principles of Psychologists and Code of Conduct, including the 2010 and 2016 amendments, effective through January 1, 2017. https://www.apa.org/ethics/code
American Association for Marriage and Family Therapy. (2026). AAMFT Code of Ethics, effective January 1, 2026. https://www.aamft.org/web/Action-Advocacy/Code-of-Ethics-New.aspx
American Counseling Association. (2014). ACA Code of Ethics. https://www.counseling.org/docs/default-source/default-document-library/ethics/2014-aca-code-of-ethics.pdf
National Association of Social Workers. (2021). NASW Code of Ethics. https://www.socialworkers.org/About/Ethics/Code-of-Ethics/Code-of-Ethics-English
Appendix A: Civil Liability, Regulatory Accountability, and Public Protection Across Provider Types
Licensed and Specialty-Certified Professionals, Certified but Unlicensed Providers, and Uncredentialed Providers
Purpose and Scope
The ethical responsibilities described in this document may have different civil, regulatory, and professional consequences depending on whether a provider is licensed, specialty-certified, both licensed and certified, or neither licensed nor certified. Licensure, certification, and the absence of credentials do not create identical duties, remedies, or enforcement mechanisms. This appendix explains the most probable forms of accountability associated with each provider category and why members of the public may receive greater protection by selecting a licensed professional who has also completed relevant specialty certification.
This discussion is educational and primarily reflects general legal principles and Oregon regulatory structures. The existence and outcome of any civil claim depend on the provider’s conduct, representations, contractual duties, professional status, applicable law, causation, damages, and the facts of the individual matter.
Why Licensure and Specialty Certification Matter
Licensure and specialty certification serve different but complementary public-protection functions. A professional license establishes that the provider has satisfied governmental requirements concerning education, supervised experience, examination, scope of practice, ethical conduct, continuing competence, and regulatory accountability. Relevant specialty certification demonstrates additional preparation in the particular risks, boundaries, methods, and ethical responsibilities associated with dating, matchmaking, coaching, and relationship services.
A licensed and appropriately certified professional is therefore subject to more extensive verification and accountability than a person whose qualifications are based only on self-description. The public may verify the professional’s license, review disciplinary information when publicly available, submit a complaint to a regulatory board, and expect compliance with legally and professionally defined standards. When specialty certification is also present, the provider has made additional representations concerning focused education and adherence to program-specific requirements.
Licensure and certification do not guarantee compatibility, safety, clinical success, or a successful relationship. They provide stronger evidence of preparation, clearer standards of conduct, defined limits on practice, and more meaningful avenues for investigation, correction, discipline, and public recourse. When services involve mental-health symptoms, trauma, intimate partner violence, suicide risk, substance misuse, impaired judgment, diagnosis, treatment, or significant emotional vulnerability, the safer and more accountable choice is ordinarily a licensed mental-health professional with relevant specialty education or certification.
Oregon-Focused Legal-Risk Analysis for Educational and Policy-Development Purposes.
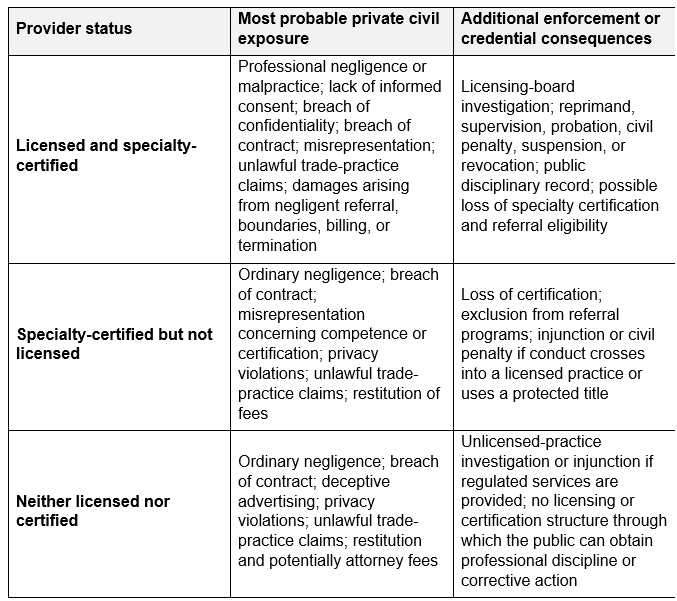
1. Licensed and certified professionals
A licensed professional is likely to be judged under a professional standard of care appropriate to the license and services actually provided. Calling the service “coaching” does not necessarily prevent a malpractice or licensing claim when the provider is functionally assessing, diagnosing, treating, managing risk, or using psychotherapeutic methods.
Likely claims include:
Failure to practice competently
Failure to recognize or respond appropriately to suicide risk, intimate partner violence, mania, substance misuse, stalking, trauma, or severe impairment
Inadequate informed consent or role clarification
Improper disclosure of sensitive information
Sexual, financial, social, or business boundary violations
Negligent referral or abandonment
Misrepresentation of credentials, outcomes, screening results, or fees
Improper insurance billing
The license creates an additional layer of accountability. Oregon boards investigate complaints involving competence, confidentiality, ethical violations, protected titles, and unlicensed practice. Available sanctions may include reprimand, required education or supervision, civil penalties, probation, suspension, or revocation. Formal discipline may become public and, for MHRA-regulated professionals, may be reported to national disciplinary systems.
Specialty certification adds a second potential consequence: revocation of certification, removal from a referral network, and a finding that the provider failed to follow standards the provider expressly represented as part of the service.
2. Certified but unlicensed providers
A private certification is not a professional license and does not authorize diagnosis, psychotherapy, clinical social work, or another legally restricted practice. Its legal significance is principally evidentiary and contractual: the provider has represented that particular education, standards, supervision, or competencies were completed.
A certified but unlicensed person may lawfully provide genuinely nonclinical education, coaching, social-skills development, or matchmaking services if the services remain within lawful boundaries and are described truthfully. However, certification will not protect the provider if the actual conduct becomes clinical. Oregon restricts unlicensed psychology and clinical social work and regulates the practice and protected titles of professional counselors and marriage and family therapists. The counselor and therapist board may seek an injunction and impose a civil penalty of up to $2,500 for each separate violation of ORS 675.825.
Probable civil claims include ordinary negligence, breach of contract, privacy violations, and misrepresentation. Certification standards may be introduced as evidence of what the provider promised, undertook, or should reasonably have known. A certification may therefore increase accountability, even though it does not create clinical authority.
3. Providers who are neither licensed nor certified
An unlicensed and uncertified person is not automatically acting unlawfully. A person may provide limited nonclinical coaching or matchmaking services if the person does not use protected titles, misrepresent qualifications, or perform activities reserved to licensed professionals.
However, lack of credentials is not immunity from liability. The person remains subject to:
Ordinary negligence
Breach of contract
Fraud or negligent misrepresentation
Privacy and confidentiality-related claims
Consumer-protection enforcement
Injunctions or penalties for unlicensed practice
Oregon’s Unlawful Trade Practices Act prohibits creating confusion about certification, approval, affiliation, qualifications, service characteristics, or service quality. A private consumer action may provide damages and, in appropriate circumstances, attorney fees; public authorities may also seek injunctions, restitution, and civil penalties.
A licensing board may still investigate an unlicensed person when the allegation involves unlawful practice or misuse of a protected professional title.
Why the public should prefer a licensed and appropriately certified professional
A license provides a government-regulated foundation: verified education, supervised clinical experience, examination, defined scope of practice, ethical requirements, continuing education, public license verification, and an enforceable complaint process. Oregon’s LPC and LMFT requirements, for example, include graduate education, supervised clinical experience, competence examinations, ethics, and Oregon law.
A rigorous specialty certification can add focused preparation that a general professional license may not provide, such as:
Distinguishing psychotherapy from coaching and matchmaking
Dating-platform privacy and information-sharing risks
Relationship screening and interpretation
Intimate partner violence and psychological-safety concerns
Conflicts created by serving both members of a potential match
Referral standards and continuity of care
Ethical advertising, outcome claims, fees, and insurance billing
The combined designation communicates two different things:
Licensure establishes lawful professional authority and public accountability. Certification demonstrates additional preparation for the particular service being offered.
Neither guarantees compatibility, safety, therapeutic success, or a successful relationship. The defensible public claim is that a licensed and appropriately certified provider offers greater verified competence, clearer ethical duties, more structured risk management, and more meaningful avenues of accountability and recourse.
For ordinary, low-risk goal coaching, a transparent and competent nonlicensed coach may be appropriate. When the service involves mental-health symptoms, trauma, risk assessment, intimate partner violence, diagnosis, treatment, or significant emotional vulnerability, the qualified recommendation is to use a licensed mental-health professional who also has relevant specialized training or certification.
Use and Legal Disclaimer
This educational document summarizes professional ethical standards and does not constitute legal advice, an official interpretation by any professional association, or a substitute for applicable statutes, administrative rules, licensing-board guidance, payer requirements, consultation, or advice from qualified counsel. Providers are responsible for determining which laws, codes, and rules govern their credentials, location, service model, and clients.